



Introduction
Iatrogenic parasitic myomas may develop after seeding by small fibroid masses when morcellation is performed during uterine surgery. This condition is the most common late complication after laparoscopic myomectomy; the reported incidence is 0.2% to 1.2% [1,2]. Several cases have described parasitic myomas that develop after abdominal myomectomy [3]. The myomas sometimes parasitize the greater omentum. Such cases are usually found only incidentally during surgery; some patients exhibit nonspecific symptoms. Acute abdominal pain attributable to torsion of the pedicle of a fibroid that has parasitized the greater omentum is extremely rare as an initial presentation [4]. However, such an event may occasionally cause acute abdominal pain.
Case report
A 38-year-old woman was admitted to our emergency department complaining of a 2-hour history of sudden, severe right lower abdominal pain. She appeared to be acutely ill. The pain was both severe and progressive. Her medical history was unremarkable. She had undergone a cesarean section 17 years prior, followed by abdominal myomectomy to remove uterine fibroids 7 months prior. During myomectomy, two intramural myomas and one subserosal myoma were removed. Uterine myomas were removed entirely without morcellation; we minimized myoma tissue disruption. The abdominal cavity contained no visible tissue remnants.
Physical examination revealed lower abdominal rigidity and guarding, with an associated rebound tenderness suggesting that surgery might be required. All vital signs were within normal ranges and the patient's consciousness was clear. The white blood cell count was mildly elevated, to 11,800/mm3, but all remaining laboratory test data were normal. Pelvic examination revealed a large, tender, non-mobile mass that filled the lower abdomen.
Ultrasonography revealed her uterus (8.6├Ś7.4├Ś6.3 cm in dimension) to contain a 4.4-cm-diameter subserosal fibroid and a 2.7-cm-diameter intramural myoma. A huge mass was evident in the upper pelvis; this extended into the upper abdomen to a position 8 cm above the level of the umbilicus. The mass was slightly heterogeneous in echotexture, and the degree of through-transmission was poor.
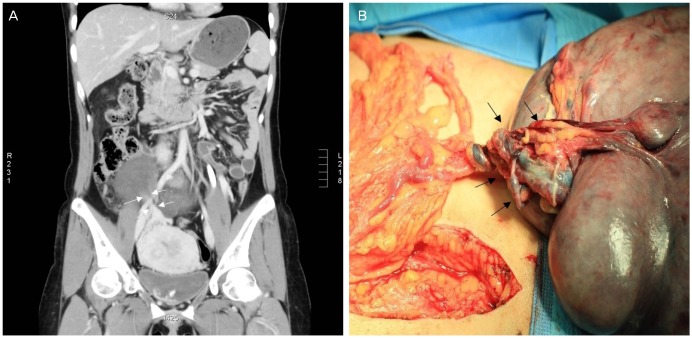
A computed tomography (CT) scan of the entire abdomen revealed a well-defined, lobulated heterogeneously enhanced mass 17├Ś15├Ś7 cm in dimension in the abdominal cavity (Fig. 1). Inferiorly, the mass lay separate from the uterus and ovaries. A small amount of fluid was noted within the pelvic cavity. The coronal CT image showed a whirling pattern of fatty streaks within the omentum (Fig. 2A). This is a relatively characteristic feature of omental torsion.
We performed an exploratory laparotomy on the basis of a preoperative diagnosis of omental torsion. During this operation, a large encapsulated mass, 17 cm in diameter, was found in the greater omentum. The mass was fed by small vessels extending from the omentum, but was nonetheless easily removed. The mass was twisted 1.5 rotations clockwise around the stalk (Fig. 2B). The operative findings were consistent with the CT data. A dark brown parasitic myoma was identified on the twisted pedicle. No other connection was evident between the omental mass and the uterus. En bloc excision of both the mass and the omentum was performed, followed by total abdominal hysterectomy due to the presence of multiple small uterine myomas.
Gross examination revealed a globular soft tissue mass 16├Ś13├Ś6 cm in dimension. The cut surface was fasciculated and dark gray in color. Histopathological examination of multiple sections revealed features compatible with a leiomyoma. The leiomyomatous tissue exhibited multifocal hemorrhages, congestion, and dilated vessels; all are typical pathological features of omental torsion. The tumor cells were immunopositive for smooth-muscle actin. These findings are consistent with the presence of an infarcted leiomyoma. Thus, we made a final diagnosis of an iatrogenic parasitic myoma complicated by omental torsion. The patient was discharged from the hospital 6 days after surgery. No abnormality was evident at follow-up 12 months later.
Discussion
Myomas are benign tumors that originate from individual smooth-muscle cells. The tumors can form wherever smooth muscle is present, but they most often develop in the uterus [5,6]. Parasitic myomas (defined as myomas caused by extrauterine seeding) were first reported in the early 1900s [7]. Traditionally, it was thought that parasitic myomas were originally pedunculated subserosal myomas that became incidentally separated from the uterus. A new blood supply was attained upon attachment and rooting to other organs [8]. However, the increasing incidence of parasitic myomas after minimally invasive endoscopic procedures may suggest otherwise [9]. Small tissue fragments retained in the abdominal cavity after morcellation are now thought to possibly explain the development of parasitic fibroids in the peritoneal cavity [9,10,11]. Such parasitic myomas are thus iatrogenic in nature.
The symptoms do not appear to be specific, but patients initially complain principally of abdominal or pelvic pain, dyspareunia, abdominal distension, an increased urinary frequency, and constipation [1,12]. Parasitic myomas develop at various sites and vary in diameter (range, 0.8 to 30 cm). The sites include the port of entry for the operation, intestines, peritoneum, omentum, and abdominal cavity [2,12,13]. The interval between the initial surgery and the repeat surgery during which myomas are discovered ranges from 2 to 108 months [12]. Several cases of parasitic myomas after abdominal hysterectomy have also been reported, suggesting that factors other than morcellation may be in play [3,14].
The present case is important in that it shows that even an abdominal myomectomy can trigger the development of a parasitic myoma. Multiple myomectomy is likely associated with myoma particle implantation in the abdominal cavity. Our surgical team carefully confirmed that no visible particles remained in the abdominal cavity after surgery. However, small particles invisible to the naked eye could have been present. Seven months later, a single parasitic myoma 17 cm in diameter was found in, and derived its blood supply solely from, the omentum. The use of a meticulous technique featuring the complete removal of even very small myoma fragments is essential during both open and laparoscopic procedures.
The omentum is rarely the source of acute abdominal pain. Torsion of the omentum is an unusual cause of such pain. The typical clinical features of omental torsion include suddenonset pain of short duration, which is usually constant initially but gradually increases in severity [15]. CT is becoming ever more important in the diagnosis of such torsion, and can differentiate surgical from nonsurgical conditions.
In February 2015, the Steering Committee on Fibroid Morcellation of the European Society of Gynaecological Endoscopy considered how parasitic fibroid development could be prevented after morcellation. Every effort should be made to prevent tissue loss and remove all tissue fragments. The patient should be placed in the reverse Trendelenburg position after morcellation and the abdomen and pelvis should be extensively irrigated after prior irrigation of the peritoneal cavity. Both the abdomen and pelvis should be meticulously inspected and any residual tissue fragments should be removed [10].
In conclusion, if a patient presents with an abdominal mass or abdominal pain after myomectomy or hysterectomy, the surgeon should be aware that an iatrogenic parasitic myoma may have formed. All necessary intraoperative precautions minimizing the development of such myomas must be taken.







")











