



Introduction
The syndrome of inappropriate antidiuretic hormone secretion (SIADH) is defined as impaired water excretion resulting in dilutional hyponatremia, leading to central nervous system symptoms [1,2]. SIADH results from a variety of medical conditions including central nervous system disorders, pulmonary diseases, paraneoplastic syndromes, and the administration of certain drugs [1,2,3].
Here, we report the case of a patient who presented with ovarian clear cell carcinoma (Ia3) and suffered from SIADH following combination chemotherapy with cisplatin and irinotecan. Cisplatin is known for its association with toxicities, primarily neuropathy and nephropathy. Although it is well known that chemotherapy drugs such as vincristine and cyclophosphamide can induce SIADH [4,5,6,7,8,9], severe hyponatremia secondary to irinotecan-cisplatin is uncommon. Hence, we briefly discuss this relatively rare case of SIADH, induced after irinotecan-cisplatin infusion.
Case report
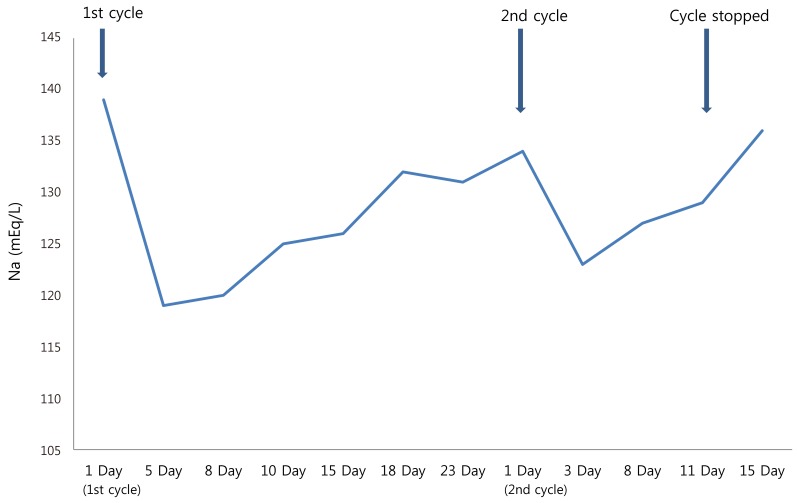
A 45-year-old woman underwent debulking surgery including total abdominal hysterectomy with bilateral salpingo-oophorectomy, omentectomy, pelvic node dissection, and appendectomy for a massive right ovarian mass (pathological staging Ia G3 clear cell type). Nine months later, computed tomography (CT) of the abdomen and pelvis revealed a slight increase in the size of the left para-aortic lymph node and newly developed peritoneal carcinomatosis. She had previously undergone 6 cycles of chemotherapy with paclitaxel and carboplatin after the index surgery on 2007. Hence, she was treated with modified chemotherapy with irinotecan on days 1, 8, and 15 along with cisplatin on day 1 for the recurrence of the disease. After 7 days of irinotecan and cisplatin administration, she was admitted to the hospital with complaints of general weakness; nausea; darkened face, palm, and nail; epigastric pain; chills; and dyspepsia. Hematological investigations revealed hyponatremia (119 mEq/L). She was treated with water restriction and drip infusion protocols until the electrolyte imbalance no longer persisted. The remaining two cycles of irinotecan were continued without cisplatin. A second cycle of irinotecan and cisplatin (day 1) was initiated after 4 weeks. A few days later, she was admitted to the hospital with signs of nausea, general weakness, and poor oral intake. Her plasma sodium concentration was 123 mEq/L, plasma osmolarity 267 mOsm/kg/H2O, and urine osmolarity 473 mOsm/kg/H2O, which were higher than the normal limit, thus confirming the diagnosis of SIADH induced by chemotherapy (Fig. 1); however, the patient remained alert. After intravenous drip infusion, her electrolyte balance was maintained. Magnetic resonance imaging of the head did not demonstrate any secondary metastases, edema, or cerebrovascular insults. Findings from the brain and chest CT performed after completion of the second cycle of chemotherapy were non-significant, but the recurrence of the cancer was evident around the abdominal area, as depicted on CT.
A new regimen of the chemotherapy including three cycles of docetaxel was started because of the elevation of tumor markers and metastases, and was continued subsequently. Irinotecan and cisplatin treatment was discontinued as the electrolyte disturbance that occurred during the chemotherapy sessions strongly suggested that they induced the SIADH.
Discussion
SIADH was first described by Bartter and Schwartz in 1967 [10]. SIADH results in hyponatremia owing to water retention caused by persistent elevated levels of arginine vasopressin or a similar peptide, despite hypotonicity of the body fluid and increased effective circulating volume [11].
Here, the patient suffered from mild symptoms such as general weakness and nausea. However, severe hyponatremia can lead to central nervous system symptoms, including confusion fatigue, seizures, coma, and even death. Thus, effort should be made to diagnose and treat SIADH, as early as possible [3].
The laboratory findings of our patient showed normal renal, adrenal, and thyroid functions. The possibility of brain metastases, cerebral edema, or cerebrovascular complications was excluded by magnetic resonance imaging, ruling out other causes of hypotonic hyponatremia [12].
There have been a few reports suggesting that SIADH is caused by cisplatin infusion. Levin et al. [13] suggested that administration of cisplatin caused SIADH; the mechanism of action may involve the alteration of central antidiuretic hormone secretion by cisplatin and also the direct effect on renal function. However, the precise basis for cisplatin-induced SIADH remains unknown. Cisplatin-related renal tubule damage is the most likely cause.
In conclusion, although SIADH following irinotecan-cisplatin infusion is an uncommon event, clinicians should be well aware of the possibility that chemotherapy administration including irinotecan-cisplatin may cause SIADH, and monitor electrolyte balance carefully.






")











