Vertical distance between umbilicus to aortic bifurcation on coronal view in Korean women
Article information
Abstract
Objective
To evaluate the vertical distance between umbilicus to aortic bifurcation on coronal view in Korean women and their relation with body mass index (BMI) and woman's age.
Methods
This retrospective study included 257 women who visited emergency center at university-based hospital from January to December 2011. All women underwent abdomino-pelvic computerized tomography (CT) due to various symptoms in a supine position. By using the electronic coronal CT images, the vertical distance between umbilicus and aortic bifurcation was measured. If aortic bifurcation was located below umbilicus, the distance was expressed as minus value (i.e., caudal to umbilicus). Age of woman, body weight, height and calculated BMI (kg/m2) were also recorded.
Results
Aortic bifurcation was located caudal to umbilicus in 52.9% and cephalad to umbilicus in 37.4%. The vertical distance had a negative relationship with BMI (r=.0.180, P=0.004), as well as woman's age (r=-0.382, P<0.001). However, a multivariate analysis revealed that the vertical distance had a significant negative relationship with woman's age (P<0.001) but not with BMI (P=0.510). An equation could be drawn to estimate the vertical distance by using woman's age and BMI: vertical distance (mm)=12.6-0.3×(age)-0.2×(BMI).
Conclusion
The vertical distance from umbilicus to aortic bifurcation on coronal view showed a significant inverse correlation with woman's age, however, the distances varied widely. Most older or obese Korean women had aortic bifurcation caudal to umbilicus.
Introduction
As laparoscopic operation is performed increasingly for abdominal and pelvic surgery, its potential for complications must be clearly understood [1]. Laparoscopic entry is of primary importance in laparoscopic surgery because of its potential association with serious complications such as visceral and vascular injuries. Although major vascular injuries are unusual, when they occur, the consequences are often serious [2,3]. In addition to substantial blood loss, continued insufflation of air after the inadvertent puncture of a large vessel can result in gas embolism, a potentially fatal sequelae [4]. The incidence of major pelvic vascular injury during laparoscopic operation is reported to be varied between 0.1% and 0.25% [2,5]. Choice of the best method for accessing peritoneal cavity depends on patient phenotype, abdominal wall morphology, and anatomic configuration of underlying vital anatomy.
Vessel injury occurs most commonly while gaining intra-abdominal access during insertion of the Veress needle and port trocars through the abdominal wall [6,7]. Injury to one or more major vessels can quickly result in fatal exsanguinations, with a majority of these deaths occurring within the first 24 hours of surgery [8]. Despite decades of research and development in an effort to create safer instruments, the incidence of these injuries has not been decreased [6,7].
Based on two presumptions that the aorta and inferior vena cava bifurcate before entering the pelvic cavity and the aorta bifurcation is usually located just below umbilicus, it was traditionally recommended to insert primary umbilicus port at a 45-degree angle to the pelvis [9,10]. However, relative locations of aorta bifurcation to umbilicus may vary in person-to-person. It was previously reported that more obese women have aorta bifurcation located more cephalic to umbilicus [7,11,12].
If this is true, primary umbilicus port insertion at a 90-degree angle can be safe in obese women. Whereas the main benefit of perpendicular entry is to minimize the chance of preperitoneal insufflation, someone recommended this method only in obese women, in whom preperitoneal insufflation is more likely to occur [13,14].
Considering vascular injury is a major cause of laparoscopic operation-related death, identification of regional relationship between umbilicus and aortic bifurcation is important. However, few studies examined the anatomic association between umbilicus and underlying retroperitoneal vessels [7,9,15].
Moreover, the normative data of the distance has never been reported in Korean women. Here we evaluated vertical distance between umbilicus and aortic bifurcation by using coronal images of computerized tomography (CT) in Korean women.
Materials and methods
Two hundred fifty-seven women who visited emergency center at the Seoul National University Bundang Hospital from January to December 2011 were selected. The Institutional Review Board of our hospital approved the use of the patients' medical records. All women underwent abdomino-pelvic (CT) due to various symptoms in a supine position. The distance between the umbilicus and aortic bifurcation was measured by using the electronic coronal CT images (Fig. 1). The center of the umbilicus was used as a reference point. If aortic bifurcation was located below umbilicus, the distance was expressed as minus value. Women who had large intra-abdominal tumors (8 cm or more in diameter), ascites, or gross anatomical deformities were excluded because these might cause dislocation of umbilicus and/or aortic bifurcation.
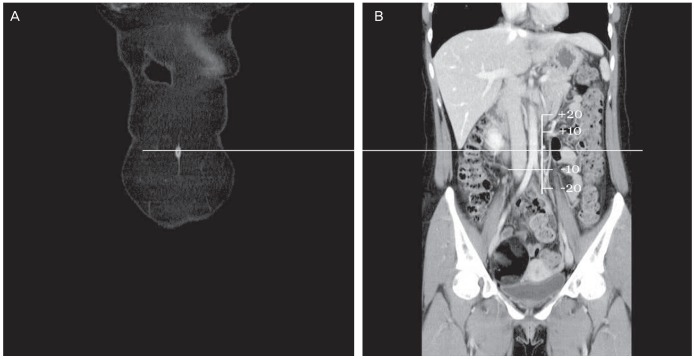
Method to measure the vertical distance between the umbilicus and aortic bifurcation by using the electronic coronal computed tomography images. After marking the center of the umbilicus (A), consecutive images are tracking until aortic bifurcation appears (B), and then the distance from the extension line of umbilicus and aortic bifurcation is measured as unit of millimeter. If aortic bifurcation is located below umbilicus, the distance is expressed as minus value. Approximately 5 cm sized mature cystic teratoma is seen on right ovary in this woman, but this case is included because relatively small tumor within pelvis does not cause dislocation of umbilicus and/or aortic bifurcation.
Patients' data including age of woman, body weight, height and calculated body mass index (BMI, kg/m2) were recorded. The body weight and height were recorded if they were measured within 10 days before checking abdomino-pelvic CT. The mean (±standard deviation) age of the patients was 44.4 (±20.8) years, ranged from 8 to 93 years. The mean height was 157 (±7.3) cm, the mean body weight was 54.5 (±9.7) kg, and the mean BMI was 22.0 (±3.6).
The PASW ver. 18.0 (SPSS Inc., Chicago, IL, USA) was used for statistical analysis and the results were considered statistically significant at P-value of <0.05. The correlation between the vertical distance and BMI was quantified using Pearson's coefficient and determined by constructing fitted curve of data plotted on linear axes. The slopes of the resulting lines were tested for statistically significant difference from zero by obtaining their P-values from the tables of critical values for the corresponding correlation coefficients.
Results
The vertical distance between umbilicus and aortic bifurcation on coronal view ranged from -51.0 mm to +36.1 mm (mean ± SD, -4.6±16.6 mm; median, -4.3 mm; 25th percentile, -15.7 mm; 75th p, 6.6 mm). Aortic bifurcation was located caudal to umbilicus in 52.9% and cephalad to umbilicus in 37.4% of the women. Twenty-five women (9.7%) had aortic bifurcation at the level of umbilicus.
Univariate analysis showed that the vertical distance have a significant negative relationship with woman's age (r = -0.382, P < 0.001) (Fig. 2A). The vertical distance also had a significant negative relationship with BMI (r = -0.180, P = 0.004) (Fig. 2B). As expected, woman's age had a significant positive correlation with BMI (r = 0.379, P < 0.001). A multivariate analysis revealed that the vertical distance had a significant negative relationship with woman's age only (P < 0.001) but not with BMI (P = 0.510). Three equations could be drawn to estimate the vertical distance (mm) by using women's age and/or BMI: 1) vertical distance = 13.9-0.8 × (BMI), 2) vertical distance = 8.9-0.3 × (age), 3) vertical distance=12.6-0.3 × (age)-0.2 × (BMI).
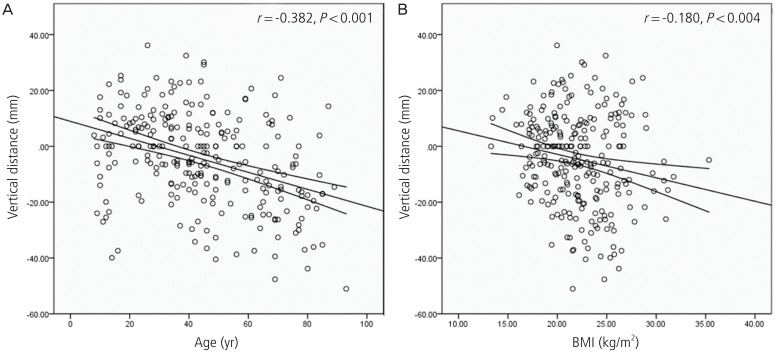
A linear regression line to show a negative correlation between vertical distance (umbilicus-to-aortic bifurcation) and woman's age (A) or body mass index (BMI) (B). The minus values indicate that aortic bifurcation located caudally to umbilicus.
Subjects were divided into five groups according to the Asian criteria of obesity (Table 1). In overweight, obese, and very obese women, the entire mean and median values of the vertical distances had minus values, indicating that most women had aortic bifurcation located caudal to umbilicus. Indeed, 66.7% of overweight, 53.3% of obese and 100% of very obese women had aortic bifurcation caudal to umbilicus.
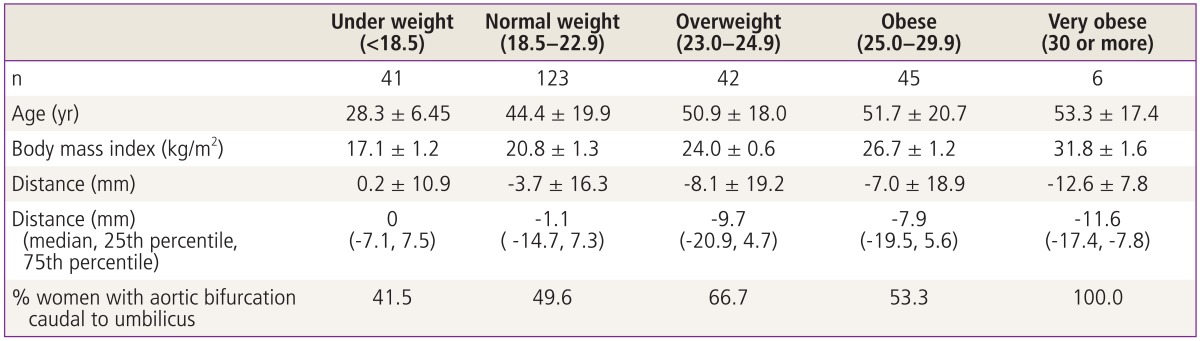
Mean age, body mass index and vertical distance between umbilicus and aortic bifurcation according to the Asian criteria of obesity
Table 2 shows the mean and median values of vertical distance between umbilicus and aortic bifurcation according to age category. The majority of the women aged 40 years or more had aortic bifurcation caudal to umbilicus.

Body mass index and vertical distance between umbilicus and aortic bifurcation according to age category
Discussion
Traditionally it has been known that more obese women has aortic bifurcation cephalic to umbilicus [7,11,16]. However, in the present study, more obese woman had her aortic bifurcation caudal to the umbilicus. Moreover, the vertical distance from umbilicus to aortic bifurcation on coronal view was more related with woman's age than BMI. The reason for this discrepancy is largely unknown. Racial difference or ethnic variability might be presumed in abdominal wall anatomy. According to our finding, surgeons should keep in mind that the aortic bifurcation is usually more caudally located in overweight/obese or older Korean women. Nonetheless, this anatomic relation showed quite severe variance according to woman's age or BMI preventing a generalization.
In a practical point of view, it has been recommended that angle of Veress needle or primary trocar differ according to patient weight; at 45-degree in normoweight, 45-degree to 90-degree in overweight, and 90-degree in the obese women. If these strategies are adapted to overweight or obese Korean women, it may result in a higher risk for great vessel injury at the time of primary insertion because aortic bifurcation is usually more caudally located to umbilicus.
To limit the incidence of vascular injury, several randomized trials were performed and showed the superiority of laparoscopy with peritoneal insufflation against "gasless" laparoscopy [16]. Combined with peritoneal insufflation by means of a Veress needle, the blind trans-umbilical insertion of the first trocar is the most widely used technique by gynecologic surgeons. However, this blind method should be cautious in a slim woman because of its proximity of the large vessels. An alternative option is Hasson technique, namely open-access method; this method has been reported to reduce the great vessel injury than blind method [17]. However, a large series study involving 10,840 women denoted six bowel injuries by this open method, of which two cases were recognized later after completion of operation [18]. Therefore, open method does completely not prevent the risk of bowel or vascular injury, thus needs more safe method to access to the peritoneal cavity [19].
A potential limitation of the present study may be absence of data about the relative dimensions of abdominal wall thickness and distance between anterior peritoneum and aorta. A recent report indicates that distances of skin to rectus sheath or to anterior peritoneum or to retroperitoneal vessels, estimated by axial images of magnetic resonance imaging, are significantly correlated with BMI [17]. However, those distances could be changed at the time laparoscopic entry because most surgeons elevate forcefully the skin around the umbilicus [18]. Moreover, personal elasticity of abdominal wall could have some effect on those distances.
A possible limitation of the present study is that the study subjects were not those destined to receive laparoscopic surgery. They visited emergency center due to various symptoms such as abdominal pain leading to abdomino-pelvic CT. However, to our knowledge, this is the first report demonstrating a significant inverse correlation between the vertical distance (umbilicus-to-aortic bifurcation) and age or BMI in Korean women. This information may be valuable for laparoscopic surgeons to insert Veress or primary trocars.
Notes
No potential conflict of interest relevant to this article was reported.