


Introduction
Most cases of inguinal hernia containing an ovary and fallopian tubes reported to date occurred in infants and were often accompanied by other congenital anomalies of the genital tract [1]. However, inguinal ovaries can occur rarely in adult women without any other genital anomalies. Moreover, inguinal ovary accompanying other ovarian diseases is extremely rare. Ozkan et al. [2] reported the only case of inguinal ovary with other ovarian pathology in which a right sliding indirect inguinal hernia containing a paraovarian cyst and fallopian tube was noted. In addition, inguinal hernia containing endometriosis is extremely rare [3,4]. Herein we report a case of an indirect inguinal hernia containing endometriosis, an ovary, and fallopian tube in an adult woman without genital anomalies, which was successfully repaired laparoscopically using polypropylene mesh.
Case report
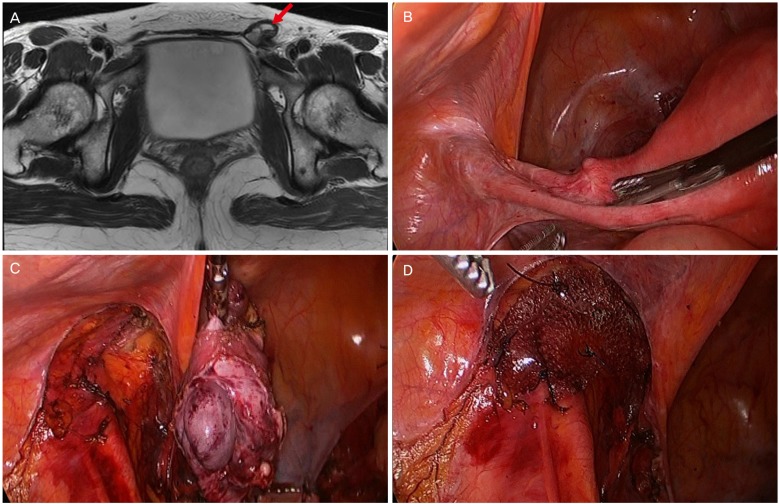
A 44-year-old multiparous patient was scheduled to undergo total laparoscopic hysterectomy for the treatment of microinvasive cervical cancer. She reported a lump in the left groin that became more apparent during menstruation, movement, and constipation. She had no specific medical or surgical history. Moreover, no genital anomalies were found on physical examination. A magnetic resonance imaging (MRI) examination of the pelvis demonstrated a 4├Ś3 cm cystic structure in the left inguinal area (Fig. 1A).
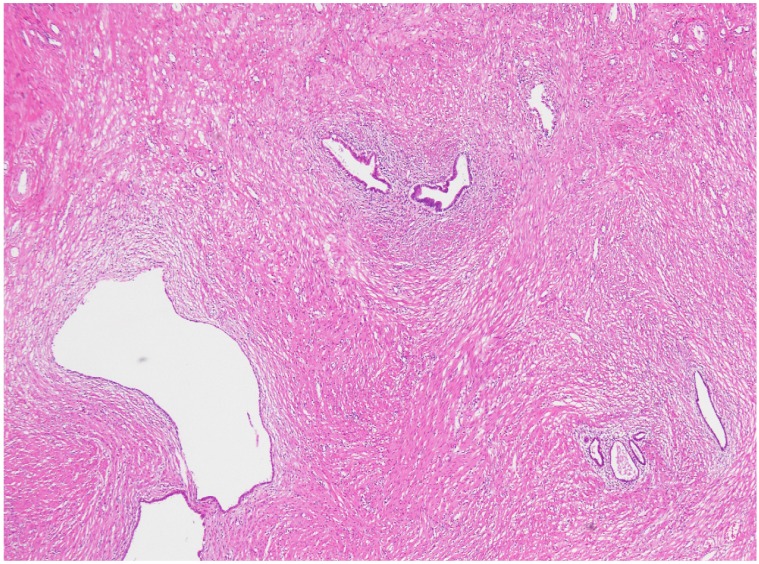
The intervention was performed laparoscopically. The uterus and right ovary, fallopian tube, and round ligament appeared normal. However, the left ovary and a portion of the left fallopian tube were herniated through the inguinal canal (Fig. 1B). After the left ovary was mobilized, the left adnexa was removed. Furthermore, a defect of the parietal peritoneum in the inguinal internal ring area was identified (Fig. 1C). Polypropylene mesh was used to repair the hernia and was anchored to the anterior abdominal wall as well as Cooper's ligament using laparoscopic sutures to prevent migration (Fig. 1D). Finally, the peritoneal flap was closed over the mesh by suturing to prevent adhesion of the intra-abdominal structures to the mesh. The patient had an uneventful postoperative course and was discharged on day 3. A histopathological examination confirmed the presence of endometriosis containing endometrial glands, with stromal cells and scattered hemosiderin-laden macrophages within fibroadipose tissue (Fig. 2).
Discussion
The inguinal canal in females not as well demarcated as in males. Several different structures normally pass through it, including the round ligament of the uterus, a vein, an artery from the uterus that forms a cruciate anastomosis with the labial arteries, and extra peritoneal fat [5]. Most cases of inguinal ovary have been reported in pediatric patients with other genital tract anomalies [1]. Inguinal ovaries in adult women are rarely reported; in fact, only 12 cases were identified in a recent review article [6]. In a retrospective review of 1,950 cases of inguinal hernia, ovaries and fallopian tubes accounted for 2.9% of the unusual contents of hernia sacs [2]. Okada et al. [7] suggested a hypotheses for this type of inguinal hernia: weakness of the broad ligaments or ovarian suspensory ligaments can contribute to ovarian herniation into the inguinal ring. This can be aggravated by high intra-abdominal pressure caused by lifting heavy objects or constipation.
Inguinal endometriosis is also a rare condition. Candiani et al. [8] reviewed 958 patients with endometriosis and reported that only 0.6% of them had inguinal endometriosis. Furthermore, only a few case reports have demonstrated an inguinal ovary accompanied by endometriosis [3,4]. A differential diagnosis is essential in cases of suspected inguinal masses. Computed tomography, MRI, and ultrasonography are useful diagnostic tools; however, MRI is more accurate than computed tomography for the detection of inguinal endometriosis [9].
Most cases of inguinal ovary and endometriosis are managed by wide excision [1,2,8,9]. Only a few case reports have described laparoscopic management for the treatment of inguinal ovary or endometriosis [6,10]. The laparoscopic approach may be suitable for patients in terms of fast recovery and cosmetic outcomes. In addition, collaboration with general surgery department is important to prevent recurrence of inguinal hernia.
In conclusion, we report a case of inguinal ovary with endometriosis. In this case, a laparoscopic approach was successfully performed and had the advantages of fast recovery and a favorable cosmetic outcome; therefore, the laparoscopic approach should be considered for the treatment of inguinal ovary with endometriosis.






")











