



Introduction
The first case of ectopic pregnancy of cesarean scar in the medical literature was reported in 1978 [1]. The incidence is variable, ranging from 1:1,800 to 1:2,216 pregnancies [2]. The recurrent form of cesarean scar pregnancy (CSP) is rarer, with only 3 case reports to date [3,4,5]; therefore, the real incidence is unknown. Some reported treatment options for recurrent CSP are based on invasive surgical methods such as aspiration and suction and curettage, except for 1 case using intra-gestational sac (GS) methotrexate (MTX) injection. We reported the fourth case of the recurrent CSP worldwide and the first to be treated with concomitant intra-GS MTX potassium chloride (KCL) injection and systemic MTX injection. In addition, we reviewed the relevant literature.
Case report
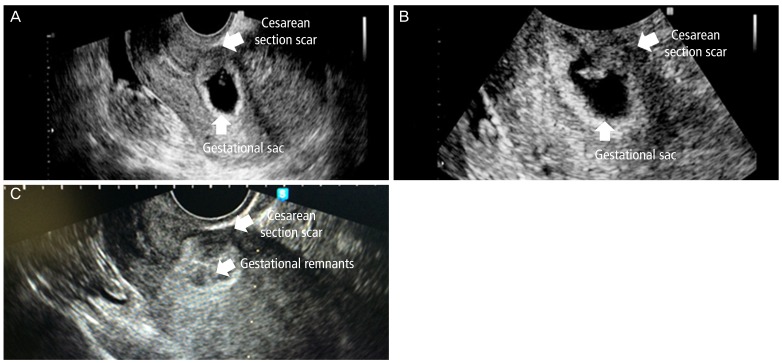
A 36-year-old, gravida 1, para 1, female came to the hospital due to CSP at 9 weeks of amenorrhea. On ultrasonography, we detected a growth GS including fetal pole sized 0.54 cm in the previous cesarean scar of the lower segment in the anterior uterine wall (Fig. 1A, B). The fetal heart rate was 96 beats per minute. Both adnexa and cul-de-sac had non-specific findings. The initial serum β-human chorionic gonadotropin (β-hCG) level was 44,419.0 mIU/mL.
She had a history of CSP at amenorrhea 5 weeks and 4 days, 10 months prior, after cesarean section for fetal distress, with oligohydramnios. At that time, the initial serum β-hCG level was 10,179.7 mIU/mL. Briefly, the treatment course included an initial intra-GS 1 mL KCL injection. Serum β-hCG level was elevated even after KCL treatment (Fig. 2A). Subsequent 73 mg MTX (50 mg/m2) injected intramuscularly appeared effective. However, for the next 10 days, serum β-hCG level was not decreased as much as expected and an intra-GS injection of 50 mg MTX was administered. On day 22 post intra-GS KCL injection, additional intramuscular 73 mg MTX (50 mg/m2) was injected and the patient recovered.
The patient was counseled with available treatment options for the current recurrence. She did not have a pregnancy plan and desired non-surgical treatment. Because multiple separate intra-GS and systemic MTX were needed in the previous CSP, we decided to treat with intra-GS MTX and KCL injection and systemic MTX concomitantly. The patient was sedated with 50 µg fentanyl and 2.5 mg midazolam. Seventy-three mg MTX (50 mg/m2) was injected intramuscularly with simultaneous injection of 2 mL KCL into the embryo; in addition, 50 mg MTX was administered into the GS after the GS fluid was aspirated with a needle (20 gauge; Neurotic Nerve Block Needle, Hakko, Nagano, Japan) under ultrasound-guidance. The fetal heart beat disappeared immediately after the procedure (Fig. 1C). The procedure took 30 minutes. The patient was discharged on the same day without any complications or complaints. However, on day 6 after first treatment, the β-hCG level was elevated. Hence, intramuscular 73 mg MTX (50 mg/m2) was injected again. On day 108 post concomitant treatment, the β-hCG level was 39.9 mIU/mL (Fig. 2B) with minimal gestational remnants on ultrasonography. The patient has been closely followed up in the outpatient clinic without complications.
Discussion
This was a case of recurrent CSP that was successfully treated with a concomitant intra-GS MTX-KCL injection and systemic MTX reported worldwide; and the fourth case of treatment of recurrent CSP, worldwide at the time of report.
The symptoms and physical findings of CSP are similar to those of other ectopic pregnancies, such as cervical and tubal pregnancies. Sonographic finding is important and the ultrasonographic diagnostic criteria include an empty uterus, an empty cervical canal, the GS located in anterior uterine wall, and prominent peritrophoblastic flow [6]. The ultrasonographic findings of our case met these criteria.
In 2004, Seow et al. [3] reported recurrent CSP in a case of a triplet pregnancy with a twin pregnancy in intrauterine cavity and 1 CSP. In their case, transvaginal sono-guided aspiration of the GS contents of the CSP was performed at 5 weeks and 5 days of gestational age. However, the remnant placenta of CSP was fused with the normal placenta of remained twin pregnancy and progressed to placenta accreta. Finally, cesarean hysterectomy was performed due to uncontrolled bleeding from the placenta site at 32 weeks of gestational age.
In 2005, Hasegawa et al. [4] reported the second case, which recurred in 6 months, successfully treated with MTX injection into GS at 9 weeks of gestational age. In this case, the MTX treatment was already successfully done at the time of diagnosis of the first CSP at 12 weeks of gestational age. But Hasegawa et al. [4] suggested that surgical management might be a preferable option for patients with first CSP, if the patients wish to become pregnant in the future. There are several case reports on surgical treatment at the first CSP, however, not recurrent CSP. For example, in 2004, Maymon et al. [7] reported emergency laparotomy and excision of the pregnancy site in the cesarean scar. In 2006, Lee et al. [8] reported the excision of CSP with laparoscopic surgery. In addition, Park et al. [9] reported the treatment of CSP by transvaginal hysterotomy in 2008.
In 2006, Ben Nagi et al. [5] reported the third case of recurrent CSP. Interestingly, 3 consecutive CSPs were diagnosed in their case. The first treatment was laparoscopy and suction evacuation at 12 weeks of gestational age and, 10 months later, the second treatment was suction and curettage at 7 weeks of gestational age without complication. Six months later, the final treatment was surgical removal at 4 weeks of gestational age without complications; and 3 months later, a laparotomy was performed to repair the uterine-scar defect. After the operation, the patient had 2 normal intrauterine pregnancies. However, both pregnancies aborted spontaneously at 7 weeks and 8 weeks of gestational age, respectively. Ben Nagi et al. [5] indicated that laparotomy for uterine repair may be useful in recurrent cases of CSP for the subsequent normal intrauterine pregnancy. We agree with their suggestion that a laparotomy in the first event of CSP could result in post-operative abdominal adhesion that can cause subfertility.
A separate treatment of intra-GS MTX or systemic MTX might fail because of the poor vascularity and surrounding fibrosis in the recurrent case [5]. In agreement, the intra-GS MTX injection did not work at the first CSP in our case; therefore, we chose the concomitant intra-GS and systemic MTX treatment at the recurrent CSP that was effective. McKenna et al. [10] previously reported a case that was successfully treated with simultaneous intra-GS MTX without KCL and systemic MTX at the first CSP, although not recurrent CSP.
Based on our case, concomitant treatment of intra-GS MTX-KCL and systemic MTX would be a minimally invasive option with efficacy and safety. However, it had limitations such as long term follow-up period of 70 days at the first CSP and 108 days at the recurrent CSP in our case, respectively.
Future pregnancy and prevention of recurrence are the first priority to consider in the management of recurrent CSP. Furthermore, patient's pain and cosmesis must also be considered currently. In a 2002 review, Fylstra [11] suggested that upon diagnosis of CSP, laparotomy should be considered as the first treatment choice for successful subsequent pregnancies even in the first event of CSP. This concept differs from ours and Ben Nagi et al. [5]. Further cases and discussion are needed to reach a definite conclusion. In terms of cosmesis, transvaginal hysterotomy may be considered at the first CSP without guarantee of future pregnancy.
In conclusion, concomitant intra-GS MTX-KCL and systemic MTX administration was a safe and effective treatment in recurrent CSP. This treatment modality may be proposed to women who do not want more children but consider less pain and cosmesis.







")











