



Introduction
Ovarian cancer is one of the leading causes of cancer deaths among women in United States and Europe. Epithelial ovarian carcinomas (EOCs) are the most common ovarian cancers accounting for 90% of cases and primarily classified according to cell type into mucinous, serous, clear cell, endometrioid, transitional, and squamous cell carcinoma [1]. Because the symptom is not apparent until advanced disease, most EOC patients diagnosed in stage III or IV when little treatment can be done to cure this disease. Thus, it is of utmost importance to find an efficient, non-invasive, and highly specific diagnostic methods for the women presenting with pelvic masses. Biochemical markers might have these diagnostic criteria and can be useful for screening, diagnosis, prognosis, monitoring, staging, as well as the management of various cancers, including ovarian cancers [2].
Cancer antigen 125 (CA125), the most widespread marker of EOCs, is a glycoprotein encoded by MUC16 gene on chromosome 19 [3]. The expression of CA125 has been reported to be elevated in 85% of serous, 65% of endometrioid, 40% of clear cell, and 36% of undifferentiated, but it was elevated only in 12% of ovarian mucinous carcinomas [3,4]. In addition, CA125 have been reported to also increase in patients with other gynecological diseases such as myomas of the uterus, benign and borderline ovarian tumors, many non-gynecological illnesses (e.g., hepatic cirrhosis, congenital heart defects), during pregnancy, and even in 1-5% of healthy women [5,6]. Thus, CA125 alone might not be a highly specific diagnostic tool for ovarian cancer, especially for mucinous type and it is necessary to find another marker, which can better discriminate ovarian pelvic mass preoperatively and to differentiate between mucinous and other types of EOC.
Carcinoembryonic antigen (CEA) is a glycoprotein that is synthesized in fetal tissues and in some carcinomas such as colorectal carcinoma [7]. Some groups advocate utilizing CEA as a potential marker for monitoring ovarian cancer, especially when CA125 is not elevated [2]. The cells of ovarian mucinous carcinoma may resemble those of the gastric pylorus, intestine, or endocervix [1]. In recent studies of comparing primary ovarian mucinous carcinomas with metastatic colorectal carcinomas, 67-85% of ovarian mucinous carcinomas were CEA positive [8,9,10]. In addition, it has been previously suggested that CA125/CEA ratio (CCR) might differentiate between ovarian and other pelvic masses, where values >25 are most probably ovarian tumors and values <25 are most probably other pelvic masses [11]. Thus, it is reasonable to hypothesize that CCR might be a good biomarker to differentiate ovarian mucinous carcinoma from other types of EOC.
The purpose of the present study was to determine whether preoperative serum CCR might be a strong biomarker, for preoperative differential diagnosis between ovarian mucinous carcinoma and other types of carcinomas, namely serous, clear cell, and endometrioid carcinomas by analyzing serum levels from female patients diagnosed with these carcinomas.
Materials and methods
1. Patients and histology
Patients who underwent elective surgery at the Gangnam Severance Hospital between January 2008 and December 2016, were included in this study. Of the individuals with EOCs, 30 (16.8%) had mucinous, 100 (28.0%) had serous, 24 (13.5%) had clear cell, and 24 (13.5%) had endometrioid carcinoma. All EOC patients were surgically staged according to the International Federation of Gynecology and Obstetrics staging system [12]. All stage I-IV patients had staging laparotomy according to the National Comprehensive Cancer Network clinical practice guidelines.
2. Clinical and laboratory data collection
For all study subjects, CA125 and CEA levels were evaluated at primary diagnosis up to 10 days prior to surgery. CA125 and CEA were measured with electrochemiluminescence immunoassay on the Roche/Hitachi Modular Analytics E170 (Roche Diagnostics, Tokyo, Japan). Age, stage, cell types, body mass index (BMI), and parity were recorded for all study subjects. The CCR was defined as the CA125 divided by CEA.
3. Statistical analysis
Serum CA125, CEA, and CCR levels among study group (mucinous, serous, clear cell, and endometrioid type) for stage I and among the same groups for stage II-IV carcinoma were analyzed using analysis of variance post hoc tests. Receiver operating characteristics (ROC) analysis was used for specificity and sensitivity estimates. The resulting area under the curve (AUC) indicates the average sensitivity of marker over the entire ROC curve for mucinous carcinoma vs. other types of EOCs. The diagnostic values of CA125, CEA, and CCR were evaluated and the optimal cut-off values of for each parameter were determined to differentiate between mucinous carcinoma and other types of EOCs. ROC analysis was plotted to investigate the optimal cut-off values that maximized the sum of sensitivity and specificity. Statistical analysis was performed with the SPSS statistical software package, version 23.0 (SPSS Inc., Chicago, IL, USA). P<0.05 was considered to indicate a statistically significant difference.
Results
Patient's characteristics for each of the 178 cases are summarized in Table 1. The mean age of patients at time of diagnosis was 46.8 years (range 31-60), the mean parity was 1.6, and the mean BMI was 23.6.
Table 1
Patient characteristics (mean level of age, parity, body mass index) with epithelial ovarian carcinoma (n=178)
The evaluation of CA125 levels for stage I EOC patients showed that the mean CA125 for mucinous carcinoma exhibited the lowest value (44.2 U/mL) among study groups (serous: 235.0 U/mL, clear cell: 86.9 U/mL, endometrioid: 153.1 U/mL) and it was significantly lower than that of serous carcinoma (P<0.05) (Fig. 1A, left panel). Similarly, for stages II-IV group, mucinous carcinoma patients had the lowest CA125 value (176.7 U/mL), compared to serous (1,709.0 U/mL) (P<0.01), clear cell (340.9 U/mL), and endometrioid carcinoma (720.3 U/mL) (Fig. 1A, right panel).
Fig. 1
Serum cancer antigen 125 (CA125), carcinoembryonic antigen (CEA), and CA125/CEA ratio (CCR) levels in patients with mucinous, serous, clear cell, and endometrioid ovarian carcinoma. Values for (A) CA125, (B) CEA, and (C) CCR for stage I (left panel) and stages II-IV (right panel) are shown. Significant values between the groups are presented as shown. Values were considered significant when P<0.05.
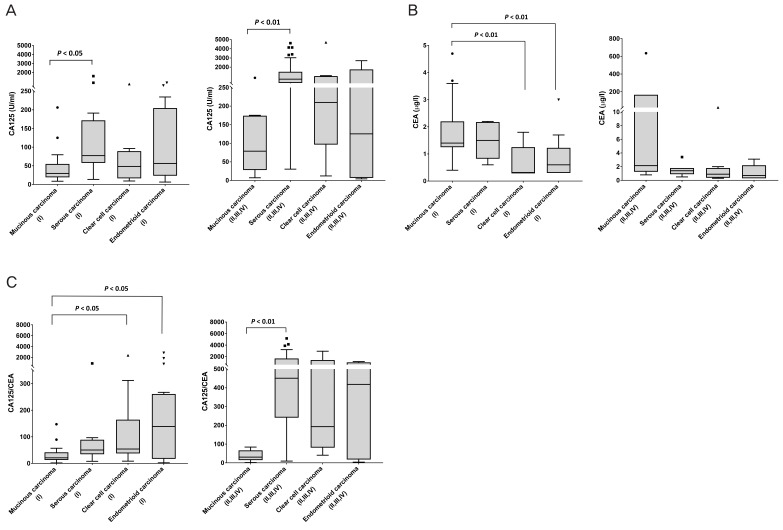
The evaluation of CEA level showed that the mean CEA in stage I mucinous carcinoma was 2.4 ng/mL, while it was 3.9 ng/mL for serous, 0.7 ng/mL for clear cell, and 1.3 ng/mL for endometrioid carcinoma (Fig. 1B, left panel). The level of CEA in mucinous carcinoma was significantly higher than that of clear cell and endometrioid carcinoma in stage I group (all P<0.01) (Fig, 1B, left panel). In stages II-IV group, the mean CEA of mucinous carcinomas (108.3 ng/mL) was remarkably highest among study groups (serous: 1.9 ng/mL, clear cell: 3.4 ng/mL, and endometrioid: 1.1 ng/mL) but there was no statistical significance (Fig. 1B, right panel).
Because the mean levels of CA125 and CEA in mucinous carcinoma were significantly different from those of other types of EOC, we calculated CCR and evaluated the diagnostic significance of CCR. Our analysis showed that CCR in mucinous carcinoma (32.1) was remarkably lowest among stage I study group (serous: 154.0, clear cell: 235.0, and endometrioid: 427.0) and there was a statistically significant difference in clear cell (P<0.05) and endometrioid carcinoma (P<0.05) (Fig. 1C, left panel). Similarly, the mean CCR of mucinous carcinoma was lowest (37.6) among study group (serous: 148.0, clear cell: 694.0, and endometrioid: 494.2) in stages II-IV and there was statistically significant difference in serous type (P<0.01) (Fig. 1C, right panel).
To further compare the utility of CCR, CA125, and CEA in differentiating mucinous carcinoma from other types of EOC, we also analyzed the ROC curve. To categorize patients as CCR positive or negative, an optimal cut-off value that maximized the sum of sensitivity and specificity in the ROC curve was used. In case of CA125 and CEA, a known cut-off value of 35 U/mL and 5.0 ng/mL was used for analysis of diagnostic power, respectively.
In case of CA125, the AUC for CCR in stage I was 0.6667 (95% confidence interval [CI], 0.9-1.0) with a sensitivity of 72.7% and specificity of 64.5%, while it was 0.8345 in stages II-IV with a sensitivity of 87.5% and specificity of 77.1% (Fig. 2A and Table 2). In case of CEA, the AUC for CCR in stage I was 0.7819 (95% CI, 0.9-1.0) with a sensitivity of 95.0% and specificity of 60.0%, while it was 0.7250 (95% CI, 0.9-1.0) in stages II-IV with a sensitivity of 83.3% and specificity of 60.0% (Fig. 2B and Table 2). We finally evaluated the CCR for mucinous carcinoma vs. other types of EOCs. The AUC for CCR in stage I was 0.7838 (95% CI, 0.9-1.0) with a sensitivity of 75.0% and specificity of 77.5%, while it was 0.9167 (95% CI, 0.9-1.0) in stages II-IV with a sensitivity of 100% and specificity of 84.4% and the cut-off value was <90.7 for mucinous carcinoma for all stages (Fig. 2C and Table 2). The positive predictive value (PPV) and negative predictive value (NPV) for CCR was 59.7% and 87.3%, respectively in stage I, while it was 14.2% and 97.7%, respectively in stages II-IV group (Table 2). Taken together, the current study suggests that the utility of CCR might be a good differentiating tool between mucinous carcinoma and other types of EOCs, supporting our hypothesis.
Fig. 2
Receiver operating characteristics (ROC) curve for preoperative cancer antigen 125 (CA125), carcinoembryonic antigen (CEA), and CA125/CEA ratio (CCR) in ovarian mucinous carcinoma vs. in other types of epithelial ovarian carcinoma. ROC curve with area under the curve (AUC) values for (A) CA125, (B) CEA and (C) CCR for stage I (left panel) and stages II-IV (right panel) are shown.
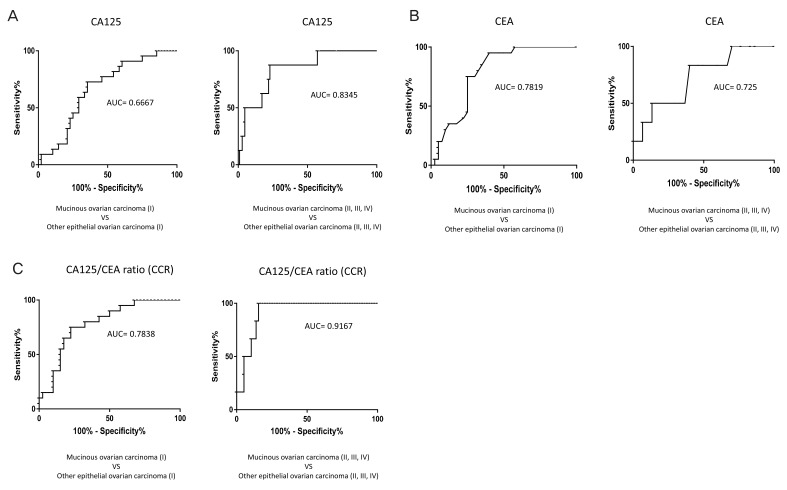
Table 2
Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and cut-off value for differentiation between mucinous carcinoma and other types of epithelial ovarian carcinoma
Discussion
Numerous tumor markers have been evaluated to improve the sensitivity and specificity of preoperative tests in patients suspected of having ovarian cancer. Among many markers, many published data have shown the usefulness of the antigen CA125, as a reliable serum tumor marker for both monitoring and following up patients diagnosed with EOC [13,14,15]. Einhorn et al. [16] reported the potential value of CA125 in preoperative diagnosis of ovarian cancers, however, controversies still exist regarding the clinical relevance of CA125 in differentiating pelvic masses [21,22,23,24]. In addition, CA125 is more often elevated in serous than in mucinous carcinomas, and while only 50% of ovarian cancers in stage I and II are associated with elevated CA125, this is found in 90% of patients at stage IIIc or IV [17,18,19,20]. Consistent with these data, our study showed that CA125 levels had the highest mean values in serous carcinoma (stage I: 235.0 U/mL, stage II-IV: 1,709 U/mL), while the lowest values in mucinous carcinoma (stage I: 44.2.0 U/mL, stage II-IV: 176.7 U/mL) in all study groups.
The several studies have demonstrated the presence of CEA in ovarian mucinous tumors and it is partly because a portion of ovarian mucinous cystadenomas contain a population of intestinal like cells that resemble those present in colonic adenomas [25]. In addition, the ovarian mucinous carcinomas contain cells that resemble those found in colonic carcinomas and, there is histochemical similarity between the mucins secreted by the intestinal type of ovarian tumors and colonic tumors [25,26]. It is therefore, not surprising that there is also a similarity in the CEA expression in the colonic tumors and the intestinal areas of the ovarian mucinous tumors. It has been known that CEA is elevated in approximately 35% of EOC patients and occurs more often in mucinous tumors (88%) than in serous tumors (19%) [27,28,29,30]. Thus, in the current study, we also evaluated the CEA levels besides CA125 in different 4 types of EOC. We found that the CEA levels in mucinous carcinoma were higher than those in other types of EOC in both stages I and II-IV group (all P<0.01), with the exception of stage I serous carcinoma.
It has been previously shown that CCR rather than CA125 alone could be a useful biomarker in the study with a larger proportion of ovarian cancer patients [11]. They also suggested that any patient referred to the hospital with an undiagnosed tumor in the pelvis should — in addition to risk of malignancy index — be tested by using the CCR <25 as a criterion for further examination [11]. In our study, because CA125 and CEA level in mucinous carcinomas were significantly different from those in other types of EOC, we hypothesized that combination of CA125 and CEA could yield a more robust and reliable tool to differentiate between ovarian mucinous carcinoma and other EOCs. In the present study, the cut-off value of <90.7 achieved high levels of sensitivity and specificity to differentiate between mucinous and other EOCs for both stage I and II-IV, but particularly for stage II-IV. Therefore, we propose to use the CCR (<90.7) as a strong preoperative diagnostic tool to differentiate between mucinous from other types of EOC.
There are certain limitations for this study such as the relatively small numbers of patients with EOC. And the preoperative CA125, CEA, CCR according to each stage (II-IV) cannot be compared between patients with mucinous carcinoma and other types of EOC. Therefore, as stage increased, preoperative CA125, CEA, CCR trends according to the increase of stage could not be analyzed in this study.
Our study demonstrates that preoperative CCR is a useful discriminative marker for mucinous carcinoma from other types of EOC. The CCR value <90.7 exhibited high specificity (stage I: 77.5%, stage II-IV: 84.4%) and sensitivity (stage I: 75.0%, stage II-IV: 100%) to differentiate ovarian mucinous carcinoma from other types of EOCs preoperatively. The CCR value <90.7 might provide a superior marker for ovarian mucinous carcinoma, especially for advanced stages (II-V) disease. Although the information obtained from preoperative CCR cannot provide all the needed information to diagnosis for ovarian mucinous carcinoma, CCR might be an important diagnostic tool to differentiate ovarian mucinous carcinoma from other types of EOCs.






")











