



Introduction
Initially described in 1983 by Steeper and Rosai [1], an aggressive angiomyxoma (AA) is an uncommon mesenchymal tumor most commonly found in the pelvic and perineal regions. The pathogenesis is unknown, although it is thought to be associated with reproduction since large percentages of AAs are estrogen and progesterone hormone receptor (ER and PR)-positive. Diagnosis is most common in women (female:male ratio=6.6:1) with a median age of 33 years [2,3]. Symptoms and presentation are typically nonspecific and often lead to initial misdiagnosis. Herein, we report our experience with robotic excision of a giant retrorectal AA with extralevator extension into the ischioanal space and extraction via Pfannenstiel incision.
Case report
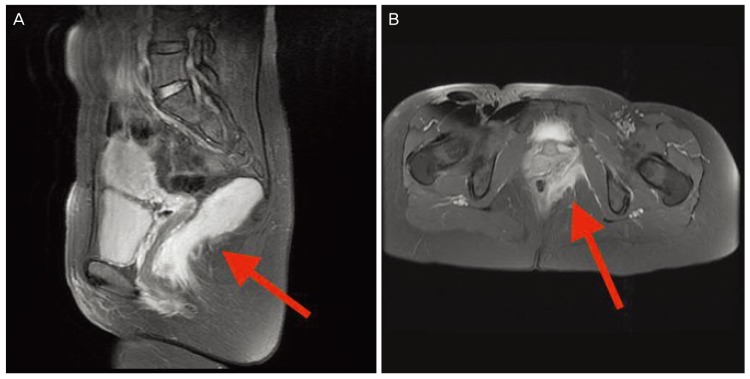
A 39-year-old Caucasian female presented with progressive pelvic discomfort and the sensation of left buttock fullness. Computed tomography revealed a retrorectal mass. High-resolution pelvic magnetic resonance imaging revealed an 8.7Ă3.5 cm complex cystic lesion in the presacral space displacing the rectum and distal sigmoid colon. The mass was noted to be intimately associated with, though not invading, the lower rectum and anus on the left side with progression between the sphincter complex and levator ani and extension into the ischioanal space (Fig. 1). Since we were not concerned about a neoplastic process, preoperative biopsies were not obtained.
Fig. 1
(A) Pelvic magnetic resonance imaging with arrow noting retrorectal aggressive angiomyxoma. (B) Pelvic magnetic resonance imaging with arrow noting retrorectal aggressive angiomyxoma extending into the ischioanal space.
A robotic extralevator excision of the retrorectal mass was performed with the Da VinciŽ Xi robot system (Intuitive Surgical Inc., Sunnyvale, CA, USA) with a 5-port technique. The patient was placed on the table in a synchronous position with both arms tucked. A chest strap was used for stability. Entry was obtained in the supraumbilical region utilizing a visible optical technique with an 8-mm AirsealŽ (ConMed, Utica, NY, USA) trocar. Two 8-mm robotic trocars (robot arms 1 and 2) were placed on the left side of the abdomen along a line horizontal to the supraumbilical trocar, all a minimum of 8-cm from each other. Another 8-mm robotic trocar (robot arm 4) was placed on the right side of the abdomen 10 cm from the supraumbilical trocar along an imaginary oblique line between the supraumbilical port and the anterior superior iliac spine. The AirsealŽ trocar was exchanged for an 8-mm robotic trocar (robot arm 3), and then placed as an assistant port superiorly and between robot arms 3 and 4. The patient was placed in a Trendelenburg position. The Da VinciŽ Xi robotic system was positioned perpendicular to the patient's left side and docked to the trocars. A 30° down robotic camera was placed in arm 3 and the pelvis was targeted. The surgical assistant was located on the right side of the table. A Small Graptor⢠(grasping retractor) was placed in arm 1, fenestrated bipolar in arm 2, and monopolar scissors in arm 4. The mass was mobilized circumferentially down to the levator muscles. Electrocautery was used to ligate the levator muscles (ileococcygeus and pubococcygeus), allowing entry into the ischioanal space. Excision was performed with the mass completely intact and it was removed via a 5-cm Pfannenstiel incision approximately 2 cm above the pubis (Fig. 2). Since the intact mass was completely removed, frozen section evaluation was not performed.
Fig. 2
Gross pathologic specimen with arrows noting the levator muscle with ischioanal fat inferiorly.
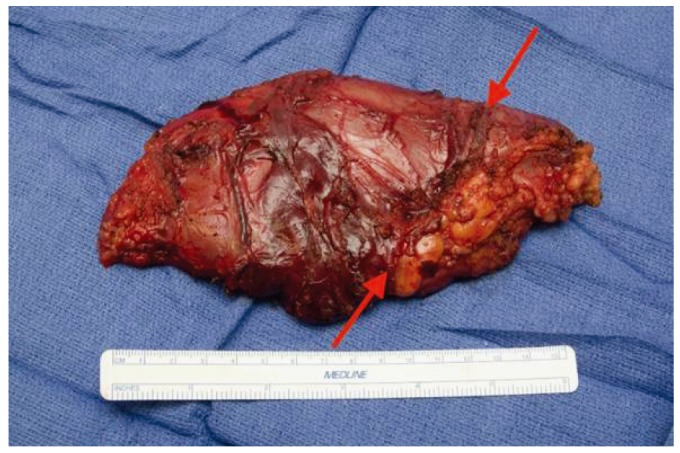
Pathological analysis revealed a 190-g, 17.7Ă9.7Ă5.8-cm, intact, oval-shaped, tan-pink, and focally yellow, myxoid mass.
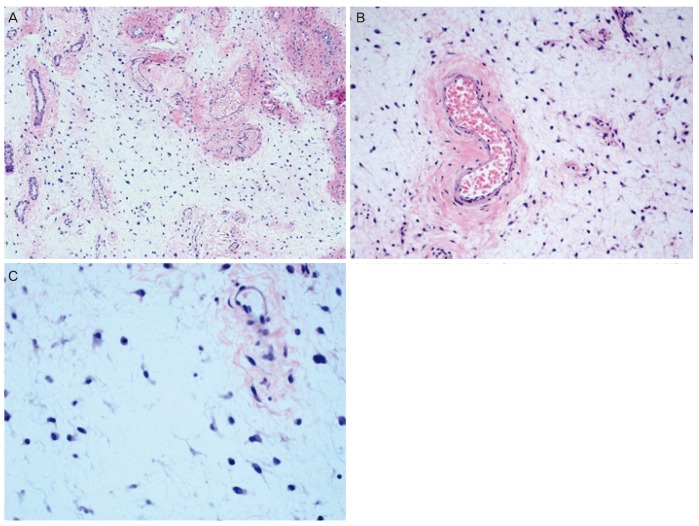
Cells were noted to be monotonous and hypocellular, composed of small spindled and stellate fibroblasts with no atypia, extremely rare mitoses, and no atypical mitotic figures. The stroma was myxoid with collagen fibers and prominent, dilated, thick-walled vessels. Tumor cells were positive for desmin, CD34, HMGA2, and actin (focal), and negative for caldesmon, KIT, DOG1, S100, and type IV collagen. The tumor nuclei were positive for estrogen and progesterone receptors with 90% of the tumor cells showing moderate to strong staining for both receptors. Findings supported a histopathological diagnosis of a giant AA (Fig. 3).
Fig. 3
(A) Microscopic low-powered histology showing monotonous and hypocellular cells composed of small spindled and stellate fibroblasts. (B) Microscopic medium-powered histology showing myxoid stroma with collagen fibers and a prominent dilated thick-walled vessel. (C) Microscopic high-powered histology showing myxoid stroma with spindled and stellate fibroblasts and no atypia.
The patient recovered without issue and was discharged the next day. Six months postoperatively, she continues to do well with no evidence of local recurrence.
Discussion
Presacral lesions are rare, with a reported incidence of 0.014% [4,5]. Retrorectal masses can be congenital, acquired, benign, or malignant (two-thirds are congenital, and two-thirds are benign) [4,5]. Although differential diagnoses are extensive, presacral tumors are broadly classified and subcategorized as benign or malignant entities. Secondary to a lack of or vague symptoms, presacral lesions are often diagnosed late. High-resolution imaging can help differentiate between benign and malignant entities, as well as provide information regarding local invasion and the overall composition of the lesion (cystic, solid, and mixed). Unless malignancy is suspected, completely cystic masses do not require preoperative biopsies, unlike most solid and heterogeneous tumors [4,5].
Histopathologically AAs are noted to be composed of myxoid stroma with collagen fibers and prominent, dilated, thick-walled vessels, which may be hyalinized with a prominent vascular smooth muscle layer. Cells are also commonly monotonous and hypocellular, composed of small spindled and stellate fibroblasts with no atypia, and have extremely rare mitoses and no atypical mitotic figures. Peripheral infiltrative margins with extension into surrounding structures (muscles, nerves, vasculature, etc.) are rarely seen. Tumor cells are most notably positive for desmin, CD34, HMGA2, and actin (focal), and negative for caldesmon, KIT, DOG1, S100, and type IV collagen. The majority of tumor nuclei will show positivity for estrogen and progesterone receptors [1,2,3].
An AA is considered a benign tumor although it can be locally invasive. Only 3 cases of distant metastasis have been reported in the literature [6,7,8]. Following complete excision with negative margins, recurrence rates can be as high as 25-47% [5]. It has been postulated that resection with positive margins does not confer a higher rate of recurrence [9]. Size of the AA does not appear to affect recurrence. Most recurrences occur within 3-5 years of extirpation. Non-operative treatment modalities, including chemotherapy, radiation, and angioembolization, have not shown benefit. Small studies have shown an advantage in treating ER- and PR-positive tumors with estrogen receptor antagonists or gonadotropin-releasing hormone agonist [10]. Due to the rarity of AA, there is no defined follow-up strategy. We are currently performing high-resolution magnetic resonance imaging of the pelvis every 6 months, with a plan to continue for at least 3 years.
Lesions below the 3rd sacral spine (S3) are considered low-lying and can typically be removed transperineally, while those above S3 require an intracoelomic approach. Tumors extending both above and below S3, as in our patient, commonly require a combined open intraabdominal and transperineal (anterior/posterior) approach for complete removal. Laparoscopic pelvic surgery is technically challenging with a steep learning curve. In addition to working in the bony confines of a narrow pelvic cavity, and in close proximity to vital structures (arteries, veins, nerves, genitourinary structures), laparoscopic surgery is also limited by technical challenges, such as 2-dimensional imaging, restricted instrument movement, poor ergonomic position, and dependence on assistants for retraction and camera movement. Robotic surgery was developed to address laparoscopic limitations by providing high resolution magnified 3-dimensional imaging, articulating endowristed instruments that mimic the movement of a hand with 7 degrees of motion, superior ergonomics, and the ability to control the camera without an assistant. Few studies have been published on the use of robotics for excision of retrorectal tumors, and none describing an extralevator approach for excision [11,12,13,14]. The robotic platform was the perfect modality for our case. The patient was spared the morbidity of incisions associated with an anterior/posterior approach and was discharged from the hospital the day after surgery.
An AA should be considered in the differential diagnosis for patients presenting with non-specific pelvic and perineal symptoms, especially in women. High-resolution imaging is imperative for operative planning. The goal of surgery should be complete excision with negative margins. Retrorectal AAs, including those with progression through the levator muscle into the ischioanal space, can be completely and safely excised with a robotic approach, which will decrease morbidity associated with abdominal and perineal incisions. Secondary to high rates of recurrence, long-term follow-up with high-resolution imaging is necessary. Few surgeons have familiarity treating retrorectal masses, and these patients are best cared for in centers with experienced surgeons.
Robotic excision of a retrorectal AA with extralevator extension into the ischioanal space and extraction via Pfannenstiel incision is technically feasible, efficacious, and safe to perform.






")











