Vaginal cancer with multiple liver and pulmonary metastases that achieved long-term survival
Article information
Abstract
Primary vaginal cancer represents only 1% to 2% of malignant neoplasm of the female genital tract. Here, we report a 68-year-old woman who showed a vaginal tumor extending to urethra and clitoris, a 10 cm-sized mass in left adnexa and multiple metastases in lung and liver. Vaginal biopsy showed squamous cell carcinoma of vagina and she was diagnosed as International Federation of Gynecology and Obstetrics stage IVB vaginal cancer. Palliative surgery including left salpingectomy, tumorectomy, and clitoris mass excision was performed. Concurrent chemoradiation therapy (CCRT) with six cycles of 5-fluorouracil and cisplatin was administered. The patient had a complete remission of 20 months after treatment. At a 40-month follow-up, there was no evidence of local recurrence or distant metastasis. We can suggest that CCRT is very effective in treating primary squamous cell carcinoma of the vagina, not only in locally advanced but also systemically involved vaginal cancer in selected cases.
Introduction
Carcinoma of the vagina constitutes only about 2% of malignant neoplasm of the female genital tract [1]. According to the International Federation of Gynecology and Obstetrics (FIGO), cases should be classified as vaginal carcinomas only after exclusion of tumors present in the vagina as secondary growths from genital or extra-genital origins [2]. Owing to the relative rarity of vaginal cancer, phase III trials have not been carried out and no consensus exists regarding optimal management. Recently, concurrent chemoradiation therapy (CCRT) has been suggested as a strategy to control locally advanced vaginal cancer [3]. To the best of our knowledge, there has been very limited data about managing primary vaginal cancer with distant metastasis. Here, we report on a patient with stage IVB vaginal cancer with pulmonary and hepatic metastases that was treated with CCRT.
Case report
A 68-year-old woman was presented with left lower abdominal pain. Her medical and family histories were unremarkable. Physical examination showed a hard mass of 4 cm diameter originating from the lower portion of the anterior vaginal wall. Biopsy revealed invasive squamous cell carcinoma of the vagina. Pap test was negative for malignant cells. Tumor marker studying including tumor antigen-4, CA-125, CA-19-9, and carcinoembryonic antigen were within normal range. On further staging, abdomen and pelvis magnetic resonance imaging (MRI) showed a vaginal tumor with invasion of urethra and clitoris and a 10 cm size solid mass in left adnexa. Positron emission tomography-computed tomography (PET-CT) and chest CT revealed multiple pulmonary and hepatic metastases (Fig. 1). Ultrasonography-guided biopsy of the left adnexa mass provided a histopathological diagnosis of metastatic squamous cell carcinoma. FIGO stage IVB vaginal cancer was diagnosed. The patient underwent palliative surgery including left salpingectomy, tumorectomy and clitoris mass excision. Due to severe adhesion, about 3 cm size remnant adnexa mass was left behind. The primary tumor at vagina was supposed to invade urethra and we decided to undergo on palliative CCRT. Microscopic pathology revealed metastatic squamous cell carcinoma involving ovary, salpinx and clitoris. The patient underwent CCRT. The major tumor and whole pelvis was treated with a total dose of 34 Gy over 17 fractions. 5-fluorouracil (5-FU) was administered at 1,000 mg/m2, in a 4-day continuous infusion schedule, combined 60 mg/m2 cisplatin (on day 1 of each course of 5-FU) for 6 cycles concurrent with radiotherapy. Follow-up abdomen & pelvis-CT taken one month after CCRT showed no evidence of tumor in vagina (Fig. 2A). Chest CT also revealed complete disappearance of multiple pulmonary metastases (Fig. 2B). After 20 months of treatment, multiple liver metastases have completely disappeared (Fig. 2C). There was also no evidence of remnant adnexa mass. A complete remission was achieved. At a 40-month follow-up, there was no evidence of local recurrence or distant metastasis.
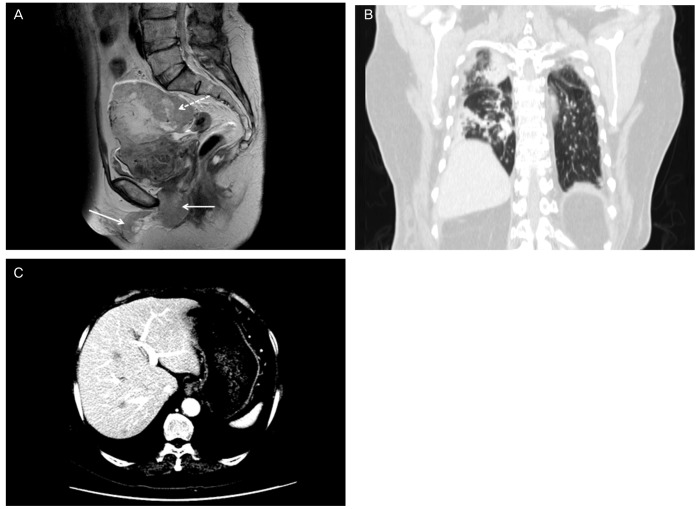
(A) Computed tomography (CT) image of the pelvis before treatment shows invasion of vaginal tumor into the clitoris (arrows), metastatic tumor in ovary (dotted arrow) and uterus. The solid arrows indicate vaginal tumor invading clitoris. The dotted arrows indicate metastatic tumor invading adnexa and uterus. (B) Multiple metastatic nodules in both lungs on chest CT. (C) Multiple hepatic metastasis in abdomen and pelvis CT.
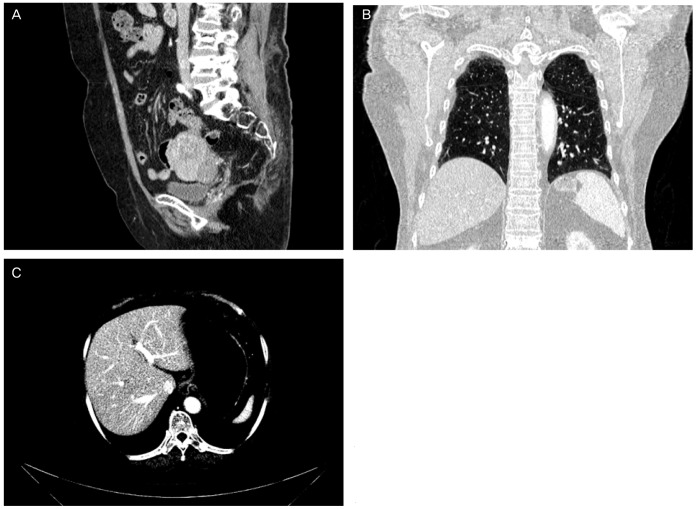
(A) Abdomen & pelvis (AP)-computed tomography (CT) taken one month after CCRT shows a complete disappearance of tumor in vagina. (B) Multiple metastatic nodules in both lungs have completely disappeared after CCRT. (C) After 20 months of treatment, AP-CT reveals a complete disappearance of multiple hepatic metastases. CCRT, concurrent chemoradiation therapy.
Discussion
Vaginal cancer is a rare entity composing only 1% to 2% of gynecologic malignancies [1]. Owing to the low incidence, randomized trials have not been carried out and current therapeutic strategies have been based on retrospective studies. Currently, radiotherapy is the most commonly accepted treatment of choice in vaginal cancer. The role of surgery has been limited to initial stages. For early stage cancers, external beam radiotherapy or even brachytherapy alone have achieved excellent results in improving 5-year survival rate. However, 5-year survival rate in advanced cases are still poor, being 52.2% for patients with stage II, 42.5% for patients with stage III, and 20.5% for patients with stage IVA disease [4]. Combination of interstitial, intracavitary, and external-beam radiation therapy is the treatment of choice for patients with stage IVA disease. Radiation is the treatment of choice for the palliation of symptoms for patients with Stage IVB disease [5,6]. Considering the similarities in histology, epidemiology, and natural history between cervical and vaginal cancers, chemotherapy concurrent with radiotherapy has been introduced to add survival benefit in patients with advanced vaginal cancers from the results of trials in patients with cervical cancers [7]. However, there is only limited reported experience with chemoradiation for vaginal cancer [3,8,9].
A few previous studies of CCRT for primary squamous cell carcinoma of the vagina have been reported. Holleboom et al. [10] reported the first case of CCRT in advanced vaginal cancer. The patient was treated with six courses of cisplatin with external radiation (40 GY to the pelvis) and interstitial brachytherapy (40 GY). After sixteen months of follow-up, there was no evidence of disease. Frank et al. [8] reported a study from the M.D. Anderson Cancer Center, that 17% of patients with stage III or IVA disease received CCRT with cisplatin-based regimens. In their study, 9 of 193 patients with vaginal cancer, 2 in stage II, 3 in stage III, 4 in stage IVA received CCRT and 44% (4 of 9) of the patients were without evidence of disease at a mean follow-up duration of 129 months [7]. More recently, 6 patients with stage II to IVA underwent CCRT in the series of Nashiro et al. [11]. The patients with stage II survived 24 months and stage III, 18 months after treatment. The remaining four were disease free at 18, 23, 33, and 55 months. They suggested that the total radiation dose can be reduced by the use of combined chemotherapy. The efficacy of CCRT cannot be determined from these limited reported experiences. However a need for further investigation in CCRT in the management of advanced disease is evident.
In conclusion, vaginal cancer is a rare malignancy which needs to be managed with experienced practitioners and specialized techniques. All treatments should be individualized based on stages of disease and performance status. CCRT should be considered as an option for treatment strategies in advanced vaginal cancer.
Notes
No potential conflict of interest relevant to this article was reported.