Misoprostol complications in second-trimester termination of pregnancy among women with a history of more than one cesarean section
Article information

Abstract
Objective
This study aims to investigate the complications due to misoprostol administration for second-trimester termination of pregnancy among women with history of 2 or more cesarean scarring.
Methods
The cohort of this retrospective study included 678 subjects who required second-trimester pregnancy termination, from 2013 to 2015 and treated with vaginal misoprostol of 100 to 400 µg. The subjects were divided into 3 groups based on their history of cesarean sections: without a history of cesarean section, with a history of one cesarean section, and with a history of more than one cesarean section and uterine scaring.
Results
The results showed that the success rate of misoprostol administration for pregnancy termination was 95.72%. The rate of bleeding as a complication was significantly higher in subjects with a history of more than one cesarean section than in other participants (risk ratio [RR], 2.24; 95% confidence interval [CI], 1.11–4.0). The incidence of uterine rupture was higher in the group with a history of more than one cesarean section than in other groups. However, no significant difference was observed between the groups (RR, 1.44; 95% CI, 0.27–7.6). There was a significant relationship between the need for other auxiliary treatments in the pregnancy termination and the history of uterine scarring (RR, 3.3; 95% CI, 1.23–9.1).
Conclusion
The present study showed that pregnancy termination using smaller divided dose of misoprostol in patients with previous history of cesarean scarring may be associated with lower incidence of uterine rupture.
Introduction
Second-trimester termination of pregnancy is increasing due to the progress in early diagnosis of fetal abnormalities and maternal life-threatening conditions [1]. In addition, with an increase in the rate of cesarean sections and other uterine surgeries, the number of women with a history of uterine scarring, who require second-trimester termination of pregnancy, is increasing [23].
Considering the increase in the number of applicants for pregnancy termination, choosing the most appropriate method is one of the most important challenges in women's health science [4]. Different methods have been proposed as options for the second-trimester termination of pregnancy. The medical abortion regimen has been widely used in replacing other methods [56]. Among the medical treatments, misoprostol is gaining popularity due to its availability and accessibility [7].
Misoprostol is a synthetic prostaglandin E1 analogue, indicated for the prevention of gastric ulcers, for the management of spontaneous abortion and also for inducing abortion [67]. The administration of this drug is a safe and effective medical method for the second-trimester termination of pregnancy [68]. Misoprostol acts as an uterotonic agent and causes contraction of uterine smooth muscle and cervical dilation [89]. However, there are possible complications with its use, such as uterine rupture, coagulation disorders, and severe, abnormal vaginal bleeding. Considerations have also been made regarding misoprostol use and its dosage for second-trimester pregnancy termination in women with previous history of cesarean section [1011].
Although uterine rupture is a serious complication with misoprostol use and is associated with high mortality and morbidity, there is a relative contraindication for the use of this drug in women with a history of cesarean section [6811]. It is still used in many medical centers. Therefore, this study attempts to assess the efficacy of misoprostol in the second-trimester termination of pregnancy, by investigating the complications of its use in women with a history of 2 or more cesarean sections.
Materials and methods
1. Patients
This retrospective cohort study was conducted among 678 subjects, referred to teaching hospitals of the Shahid Beheshti University of Medical Sciences, Tehran, Iran, during 2013–2015, who required a second-trimester termination of pregnancy through treatment with vaginal misoprostol.
The inclusion criteria were as follows: pregnant women in the second trimester with 14 to 24 weeks gestational age determined by ultrasound, and candidates for pregnancy termination due to major fetal abnormalities, fetal death, premature rupture of membranes, and other maternal indications for termination of pregnancy. The exclusion criteria were as follows: multiple pregnancy, women with classic cesarean scarring, known allergies to misoprostol, history of heart or liver disease, use of misoprostol by non-vaginal methods, and incomplete medical records.
2. Study protocol
The participants were divided into 3 groups based on their history of cesarean sections: without a history of cesarean section, with a history of one cesarean section and with a history of more than one cesarean sections and uterine scaring (any history of uterine surgery such as cesarean and myomectomy). The divided dose of misoprostol in all cases ranged from 100 to 400 µg, at intervals of 4 to 6 hours, via vaginal administration [121314].
A checklist including patient's age, gestational age, divided dose of misoprostol, total dose of misoprostol, duration of induction per hour, number of previous cesarean sections and complications, was completed by the study subjects. The recorded complications included postpartum hemorrhage (>500 mL), need for uterine packing, and hysterectomy.
The primary aim of the current study was to investigate the major complications of using misoprostol (such as hemorrhage, uterine laceration, and hysterectomy) in women with a history of 2 or more cesarean sections and in the second place, to evaluate the success rate of misoprostol use in pregnancy termination.
If 48 hours after the administration of misoprostol at a total dosage of 2,000 µg, pregnancy termination was not completed and there was no response to misoprostol, other methods could be used, including high-dose oxytocin induction (50 units oxytocin in 500 mL of normal saline infused during 3 hours; then 1-hour diuresis; then sequentially escalating in a similar fashion to 150, 250, 200, 250, and finally 300 units oxytocin, each in 500 mL normal saline) [15] or using mechanical methods (e.g. hysterotomy) which were to be performed after signed informed consent. In cases of severe hemorrhage [16] (acute uterine bleeding had been described as excessively heavy or prolonged bleeding of uterine origin, sufficient in volume as to require urgent or emergent intervention) and retained placenta, surgical evacuation of the uterus would be considered.
3. Statistical analysis
Percentages were calculated for categorical variables, and mean and standard deviation were calculated for continuous variables. Differences between the 2 groups of participants were assessed using independent Student's t-tests for continuous variables and chi-square tests for categorical variables. Risk ratio was calculated with 95% confidence interval to assess the risk of different complications in women with history of more than one cesarean section. Data were initially scrutinized for normality to conform to the assumptions of the applied parametric statistics. To assess the deference's between the mean and the proportion of the studied variables an analysis of variance or Kruskal-Wallis test was used. Further, to investigate the correlation between the 2 continuous variables, Pearson correlation coefficient test was used. The Stata software (version 13MP; StataCorp, College Station, TX, USA) was used to perform all the statistical analyses; P-values less than 0.05 were considered statistically significant.
Results
In this retrospective study, 678 subjects were studied. Out of them, 247 patients had no cesarean section (group 1), 218 patients had a history of one cesarean section (group 2), and 213 patients had a history of 2 or more cesarean sections (group 3). There was no case of placenta previa in this study. The mean age in the studied groups was 26.3±5.1, 28.8±3.8 and 28.5±4.3 years, respectively. There was no significant difference in gestational age (P-value=not significant [NS]) (Table 1).
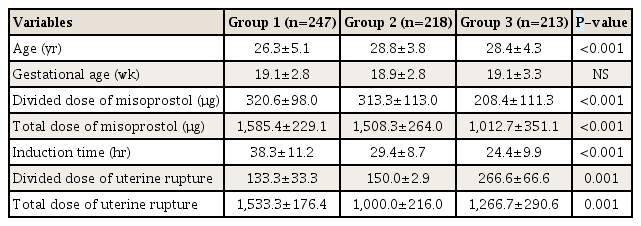
Demographic characteristics of patients
The mean divided dose of the administered misoprostol in group 1 was 320.6±98.0 μg, in participants with one cesarean section was 313.3±113.0 μg and in participants with more than one cesarean section was 208.4±111.3 μg. There was a significant relationship between the total doses of misoprostol vaginal administration in the 3 groups. The total dose of misoprostol vaginal administration in the first group was significantly higher than other participants (P-value<0.001). Total dose of misoprostol vaginal administration had a significant negative relationship with gestational age (P-value<0.001, r=−0.14). However, we found no significant correlation between the age of the subject and the total dose of misoprostol (P-value=NS). Out of the total group, 31 subjects had more than 500 mL of blood loss, and hemorrhage in subjects with more than 1 cesarean section was more than the rest of the cohort. The results showed a significant relationship between hemorrhage as a complication and the history of uterine scarring (RR, 1.56; P-value=0.04). Out of the total group, 12 participants had uterine rupture. The results showed that misoprostol was associated with hemorrhage and uterine rupture (P-value=0.04). However, there was no significant relationship between uterine rupture and the history of uterine scarring (P-value=NS) (Table 2).

Frequency and risk of clinical complications in studied subjects
The mean induction period in the group, that did not have uterine rupture, was 31.05±11.60 hours. The mean induction period in the group with uterine rupture was 30.00±9.83 hours. The mean induction period was not significantly different in the 2 groups (P-value=NS).
In addition, 95.7% of misoprostol cases did not require an auxiliary treatment and only 29 patients needed an auxiliary method, of whom 22 patients were participants with more than one cesarean section (P-value<0.001). Despite the induction of abortion through misoprostol and other auxiliary methods, 157 participants required curettage for the removal of fetal remains, of whom non-cesarean participants significantly needed curettage more than others (P-value<0.001). However, there was no significant difference between groups 2 and 3 regarding the need for curettage (P-value=NS). The results showed that 5 participants needed hysterectomy to be performed: 1 patient from group 1, 2 patients from group 2 and 2 patients from group 3. There was no statistically significant difference between the 3 groups in terms of hysterectomy (P-value=NS). However, there was statistically significant difference between subjects with or without hysterectomy, in terms of divided or total dose of misoprostol (P-value<0.001) (Fig. 1).
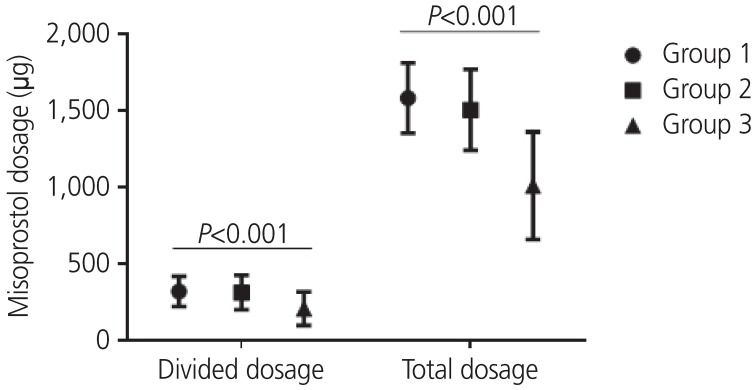
Total and divided misoprostol dosage among the different groups in this study.
Discussion
While surgical abortion is safe when done appropriately [17], many women select medical abortion, especially those at a younger age [18]. Misoprostol is a prostaglandin E1 analogue that has been primarily used for the treatment and prevention of gastric ulcer disease [61920]. However, misoprostol has been also used as an abortion-inducing agent [1921].
Various studies have explored the effects of misoprostol on the induction of spontaneous termination of pregnancy, which indicates the positive effects of this drug. However, the use of this drug is always accompanied by complications [1921]. Few studies, though, have examined the effects of the medication on labor induction in women with a history of cesarean section and uterine scarring. Studies have shown that the main complications of using misoprostol in women with previous history of cesarean section include uterine rupture, need for blood transfusion, retained placenta and surgical evacuation of the uterus, lack of response to treatment and the need for auxiliary treatment for pregnancy termination and hysterectomy. Among these complications, uterine rupture is the most dangerous and serious complication [142223].
In this retrospective cohort study, we found that medical termination of pregnancy using vaginal misoprostol alone was 95.72% effective in women with 14–24 weeks gestational age. Zikopoulos et al. [19] study showed that medical termination of pregnancy, using misoprostol alone, was 96% effective.
The results of current study showed that the mean divided dose of misoprostol in patients with more than once cesarean section was significantly lower than doses in the other 2 groups. Furthermore, the mean total dose of misoprostol was the highest in group 1 and was also the lowest in subjects group 3. In addition, the induction time in group 3 was lower than in the rest of the subjects. The results of our study showed that there is no significant relationship between uterine rupture and induction period.
Karaçor et al.'s findings [24], which were in line with our study, indicated that the total dose of misoprostol was lower for pregnancy termination in women with history of previous uterine scarring. Statistical analysis showed that there was a significant relationship between bleeding complications and history of uterine scarring. The chance of hemorrhage as a complication was greater for women with a history of more than 1 cesarean sections. They also concluded in their study that induction that lasted more than 24 hours might be associated with the risk of uterine rupture [24].
The results also showed that 4.57% of the subjects of the study lost more than 500 mL of blood during the pregnancy termination and 3.4% of them needed blood transfusion. Statistical analysis showed that there is a significant relationship between hemorrhage complications and history of uterine scarring. The chance of hemorrhage was higher in women with history of more than one cesarean section.
Daskalakis et al.'s study [13] reveals that delivery in patients with previous cesarean section has a 0.4% chance of rupture, and this probability increased if misoprostol was used in delivery induction, with or without oxytocin. The results of our study showed that the prevalence of uterine rupture in the subject group was 1.77%, thus indicating that the effect was due to misoprostol use. Considering the fact that there was no significant difference between the 3 groups in terms of uterine rupture, it was higher among patients with a history of more than one cesarean section. Dickinson and Evans [25] reported that patients with previous cesarean section had an increased risk of uterine rupture with misoprostol use. However, Iftikhar and Burney [26] reported no complications such as uterine rupture, major hemorrhage, or shock to be observed after the use of misoprostol in women with a history of one or more cesarean sections. They concluded that there were no contraindications and that misoprostol use is safe and effective [26]. Further, Naguib et al.'s findings [23] confirmed our study's conclusions.
Our results also showed that the rate of using auxiliary methods such as high dose oxytocin induction, mechanical methods, or hysterotomy for pregnancy termination was 4.28% and was significantly higher in group 3 than in other groups. It seems that uterine scarring reduces the response of uterine receptors to misoprostol and increases the need for additional approaches in pregnancy termination. In addition, 23.1% of the study subjects required curettage for the removal of fetal remains due to retained placenta or hemorrhage. The results showed that the need for curettage was significantly higher in participants without cesarean section than in those with a history of cesarean section. However, there was no significant difference between participants with one cesarean section and more than one cesarean section.
These contradictions in the results of different studies can be related to ethnic differences as well as differences in the study sample size. Therefore, further studies are required for establishing reliable results. However, it can be argued that drugs with such complications should be used with caution and careful monitoring.
The present study showed that misoprostol use in pregnancy termination did not increase the incidence of uterine rupture in patients with previous history of cesarean scarring. The major complication of misoprostol administration was hemorrhage in the groups with previous cesarean section. In addition, the rate of using auxiliary methods in the pregnancy termination was higher in groups with history of previous cesarean section.
The fact that we did not perform routine curettage or manual uterine vacuity verification after abortion, might be highlighted as a strength of our study. Indications were directed towards placental examination and blood loss evaluation. Moreover, the relatively large sample size of our study, allowed researchers to compare the different outcomes between the 3 groups (without a history of cesarean, with a history of one, and those with 2 or more cesarean sections).
The limitations of this study were related to the retrospective data gathering; therefore, the risk of information bias, such as measurement and misclassification, should be considered. It was assumed that the local regimens of Misoprostol were administered as recorded, but it is possible that some participants received additional medication, although this is unlikely. Uterine scar complications might have been missed if clinical manifestation were not found in the participants. Also, as the dosage of Misoprostol used in each group was different, it should be considered as a limitation of the current study.
The present study showed that termination of pregnancy by less divided dose of misoprostol in patients with previous history of cesarean scarring may be associated with lower uterine rupture. However, considering the incidence of uterine rupture in the group with a history of cesarean section, caution must be exercised.
Notes
Conflict of interest: No potential conflict of interest relevant to this article was reported.
Ethical approval: This study was approved by ethics committee of the Shahid Beheshti University of Medical Sciences (IRB No. REC.0313). All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Patient consent: Verbal consent was obtained by phone from all individual participants included in the study.

