Risk factors for type-specific persistence of high-risk human papillomavirus and residual/recurrent cervical intraepithelial neoplasia after surgical treatment
Article information

Abstract
Objective
This study aimed to investigate the clinicopathologic risk factors for type-specific persistence of high-risk human papillomavirus (hrHPV) and residual/recurrent cervical intraepithelial neoplasia (CIN) after surgical treatment.
Methods
Patients with CIN-2/3 who underwent conization or loop electrosurgical excision procedure (LEEP) at Korea University Hospital were enrolled. All patients underwent hrHPV testing and genotyping before conization or LEEP followed by both hrHPV genotyping and cytology. The significance of associations between patient characteristics and persistence of infection were assessed by multivariate logistic regression analyses.
Results
Among 398 women with pathologically confirmed CIN-2/3, 154 (38.7%) patients showed hrHPV persistence after surgical treatment. In multivariate analysis, high preoperative hrHPV load (P<0.05; odds ratio [OR], 2.063), presence of CIN-2 at treatment (P<0.01; OR, 2.732), and multiple hrHPV infections (P<0.001; OR, 4.752) were associated with hrHPV persistence. HPV 53 was the most likely to persist after treatment (24/43, 55.8%). The risk of residual/recurrent CIN-2/3 was higher in persistent infection with HPV 16 than other types (P<0.05). Menopause (P<0.001; OR, 3.969), preoperative and postoperative hrHPV load (P<0.05; OR, 2.430; P<0.05; OR, 5.351), and infection with multiple hrHPV types (P<0.05; OR, 2.345) were significantly related to residual/recurrent CIN following surgical treatment.
Conclusion
HPV load before treatment and infection with multiple hrHPV types were predictors of postoperative hrHPV persistence. HPV 53 was the type most likely to persist, but HPV 16 was the type that was most closely associated with residual/recurrent CIN-2/3.
Introduction
Cervical intraepithelial neoplasia (CIN) is caused by persistent infection with high-risk human papillomavirus (hrHPV) and is a precursor of cervical cancer [1]. Persistent infection with hrHPV is the direct cause of the vast majority of CINs and invasive cervical cancers [2]. Age, parity, smoking, sexual behavior, and socioeconomic status have been reported as potential factors mediating persistent infection by hrHPV [3].
The standard treatment for CINs, especially high-grade lesions, is conization or the loop electrosurgical excision procedure (LEEP) [4]. Even if the lesion is completely removed, these patients have a higher risk for recurrence of high-grade lesions compared to the general population [5]. Because of this potential risk, close monitoring after surgical treatment for CIN is standard practice. Screening for patients at risk of residual/recurrent high-grade lesions using combined testing for hrHPV with cytology has a negative predictive value of 99% [6,7]. Detection of HPV infection has been highlighted as an objective marker with high sensitivity in screening or follow-up, as there is less interobserver variability compared to cytology testing alone [8]. High-grade squamous intraepithelial lesions (HSILs) with hrHPV infection have been demonstrated to be highly predictive of invasive cervical cancer [7,9].
It is well established that persistent infection by HPV after conization is a precursor for relapse of CINs. Patients tested as HPV- after conization had a 6.5% risk of residual/recurrent high-grade lesions, while those tested as HPV+ had a 60.9% risk [10]. Determining the characteristics and risk factors for HPV persistence after CIN treatment has implications for the early detection and treatment of high-grade lesions and cervical cancer, as well as for our understanding of the natural history of HPV infection. Several studies have analyzed persistent infection by HPV and residual/recurrent CINs after conization or LEEP [3,11-14]. However, specific HPV genotypes have different natural histories, and individual phylogenetic species have different carcinogenicities. In terms of HPV persistence, therefore, a detailed analysis of specific HPV genotypes can help expand our understanding of the nature of HPV infections [15].
In this study, we aimed to analyze genotype-specific persistence of HPV and persistence/recurrence of CIN after surgery in patients that underwent hrHPV genotyping before and after conization or LEEP.
Materials and methods
1. Study population and inclusion criteria
A flowchart of participant enrollment is provided in Fig. 1. A retrospective analysis was performed on 1,029 patients who underwent conization or LEEP at Korea University Guro Hospital and Anam Hospital between January 2014 and September 2018. We included patients for whom information on HPV genotypes before and after surgical treatment was available. Of these 1,029 patients, 504 were excluded because of preoperative negative hrHPV or lack of HPV data. The remaining 525 patients were documented to have hrHPV based on the AnyplexTM II (Seegene, Seoul, Korea) HPV genotyping test before operation. Patients with histologically confirmed CIN of grade 2/3 through punch biopsy were included. Of the remaining 525 patients, 31 and 19 were excluded due to diagnosis of VAIN or CIN-1, and due to invasive cervical cancer respectively. Finally, of the remaining 475 patients, 77 were lost to follow-up for HPV DNA testing after conization or LEEP, resulting in a total enrollment of 398 patients for this study.
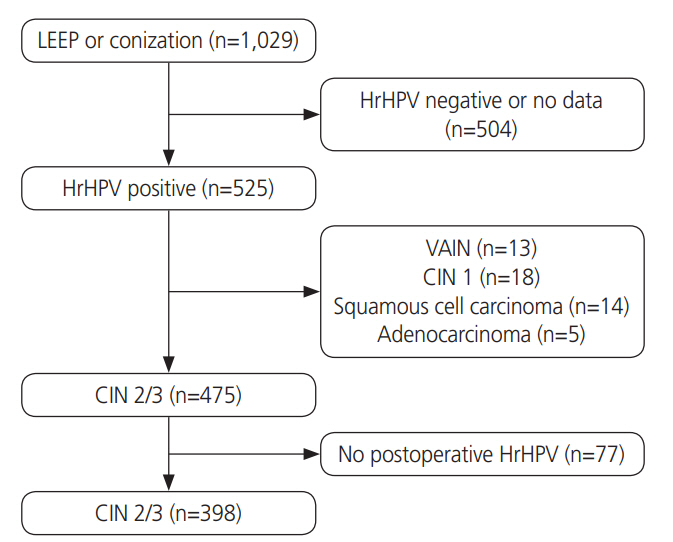
Composition of enrolled patients’ population. LEEP, loop electrosurgical excision procedure; hrHPV, high risk human papillomavirus; VAIN, vaginal intraepithelial neoplasia; CIN, cervical intraepithelial neoplasia.
Conization was performed using the surgeon’s choice of cold-knife or Bovie blade after the application of Lugols’ iodine solution to confirm previous cervical lesions. Hemostasis was then achieved with electric coagulation.
Postoperative follow-up was done between 3–6 months after surgical treatment, and follow-up visits occurred every 6–12 months thereafter. Patients underwent cervical inspections, HPV DNA genotyping tests, and cervical cytology. Papanicolaou smears were interpreted by the Bethesda system and histologic diagnoses of excised specimens were based on the World Health Organization classification.
2. Human papillomavirus (HPV) test with Anyplex™ II
We extracted HPV DNA in accordance with the manufacturer’s guidelines. Nucleic acids were extracted from 400 μL of sample using the MICROLAB STARlet automated purification system (Hamilton, Reno, NV, USA). HPV detection and genotyping were performed using an Anyplex II HPV28 and CFX96 real-time thermocycler (Bio-Rad, Hercules, CA, USA) according to the manufacturer’s instructions [16]. The Anyplex II HPV28 has been shown to perform comparably to the Roche Cobas 4800 HPV assay (Cobas) (Roche Molecular diagnostics, Branchburg, NJ, USA) and the HR Hybrid Capture 2 (Qiagen, Gaithersburg, MD, USA), which are accredited for cervical cancer screening and detection of hrHPV [16,17]. Furthermore, Anyplex II HPV28 is considered a reliable and validated test for detecting hrHPV genotypes [18].
3. Human papillomavirus (HPV) persistence and genotype-specific persistence
Persistent hrHPV infection was defined as the presence of hrHPV at the first follow-up visit after surgery regardless of HPV type. HPV type-specific persistence was defined as the presence of the same HPV type before surgery and at the first follow-up visit after surgery. Multiple HPV infections in a patient were considered separate units when analyzing the HPV type-specific persistence rate. Patients who were HPV negative at the first follow-up visit, or had cleared all HPV types present before surgery, were defined as being clear of HPV infection.
4. Statistical analysis
The Chi Square (χ2) and Fisher’s exact tests were used to evaluate the significance of differences in variables between the HPV persistent group and the HPV non-persistent group. The risk for HPV persistence was modelled by logistic regression analysis and is presented as relative risks (odds ratios [ORs]) with 95% confidence intervals (CIs). Backward stepwise multivariable logistic regression was applied to identify factors independently predictive of persistent/recurrent CIN1+ and CIN2+.
P-values (from 2-sided tests) less than 0.05 were considered significant. Data were analyzed using SPSS software (version 22.0; SPSS Inc., Chicago, IL, USA).
Results
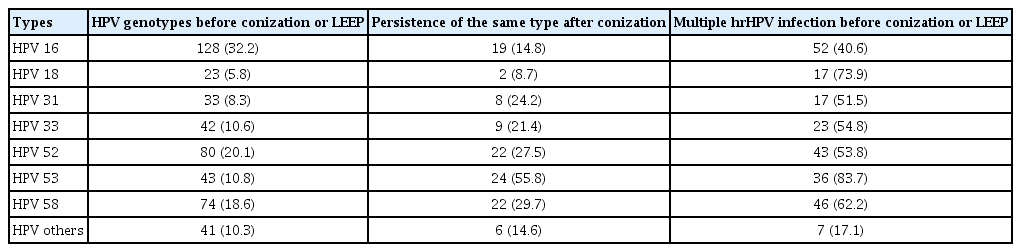
A total of 398 patients who tested positive for hrHPV and underwent conization or LEEP met the inclusion criteria. The mean number of follow-up visits was 2.8 (range 1–7) and median follow-up period was 17.3 (range 4–48) months. Overall, the prevalent hrHPV genotypes were HPV 16 (n=128, 32.2%), HPV 52 (n=80, 20.1%), HPV 58 (n=74, 18.6%), and HPV 53 (n=43, 10.8%). Two hundred thirty-six patients (59.3%) were infected by a single hrHPV type. Of the remaining 162 patients infected with multiple types of hrHPV, 118 patients (29.6%) were infected with 2 hrHPV types, 32 patients (8.0%) were infected with 3 hrHPV types, and 12 patients (3.0%) were infected with more than 4 hrHPV types.
Persistent hrHPV infection after conization or LEEP was identified in 154 patients (38.7%) of the 398 patients enrolled. Baseline characteristics of these patients are presented in Table 1. Mean age at diagnosis was 41.96±12.63 years in patients with hrHPV persistence compared to 38.37±10.57 years in those without hrHPV persistence (P<0.005). Initial results from cervical cytology were not significantly associated with hrHPV persistence (P=0.232). Among patients who did not show hrHPV persistence, 25.4% had ASCUS and 37.3% had ≥HSIL at initial cytology. However, in patients with hrHPV persistence, 26.1% had ASCUS and 32.8% had ≥HSIL. Residual/recurrent CIN2+ occurred in 15 patients (9.7%) with hrHPV persistence, while it did not occur in those without persistent infection. Both patient groups (with and without persistent hrHPV infection) were similar in terms of previous treatment for CIN, type of surgery, glandular involvement, and socioeconomic status including parity and marital status.
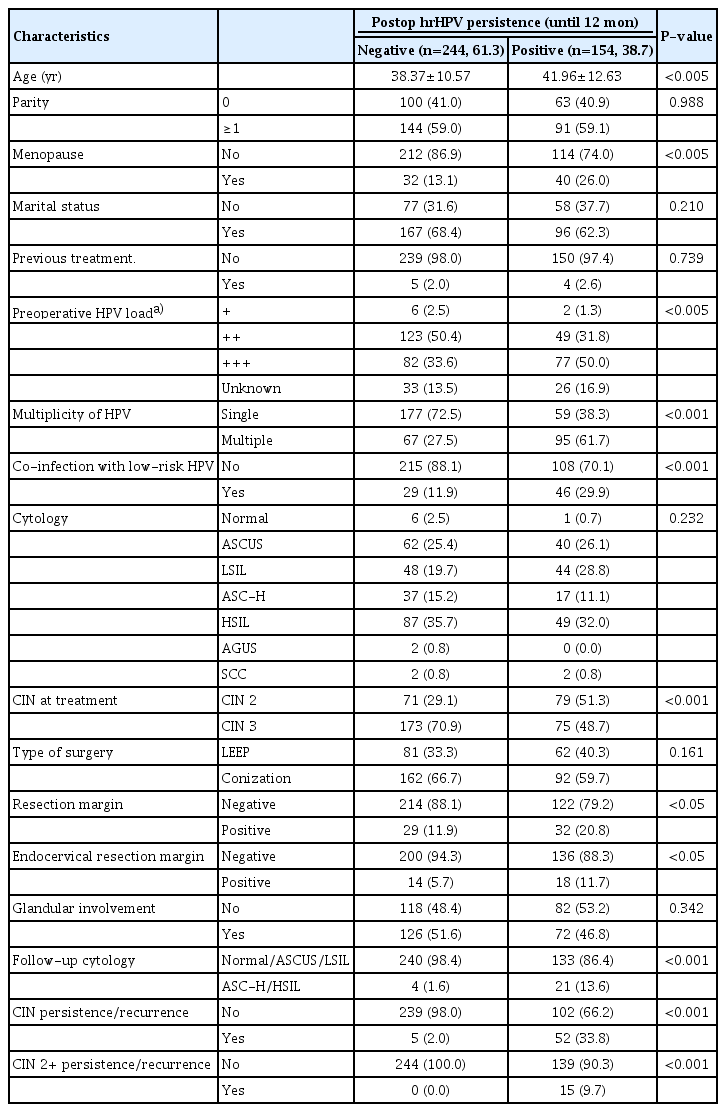
Overview of patient characteristics based on the postoperative human papillomavirus (HPV) status
Unadjusted and adjusted odds ratios for clinical factors selected for multivariable analysis are presented in Table 2. Age ≥50 years (OR, 2.553; 95% CI, 1.406–4.636; P<0.005) and post-menopausal status (OR, 2.577; 95% CI, 1.355–4.899; P<0.01) were risk factors for hrHPV persistence in univariate analysis; however, these factors were not significant in multivariate analysis (P=0.182 and P=0.912). HPV was more likely to persist in patients with CIN-2 than in patients with CIN3 (OR, 2.674; 95% CI, 1.451–5.128; P<0.01). HPV viral load at baseline was an independent predictor of persistence. HPV with a viral copy number >105 at baseline was associated with an increased rate of persistence at 12 months (OR, 2.063; 95% CI, 1.139–3.737; P<0.05). Positive resection margin was not a significant risk factor for hrHPV persistence (OR, 1.319; 95% CI, 0.558–3.121; P<0.01), although it was associated with hrHPV persistence in univariate analysis (OR, 1.936; 95% CI, 1.117–3.353; P<0.05). Furthermore, there was no significant association between hrHPV persistence and socioeconomic status, history of previous treatment, coinfection with low risk HPV, or glandular involvement.

Risk factors associated with high-risk human papillomavirus (hrHPV) persistence after surgical treatment
Type-specific persistence of hrHPV was found in 120 of the 398 patients (30.2%). Table 3 shows the rates and patterns of HPV infection according to HPV genotype. HPV 16 was the most prevalent genotype (128/398, 32.2%), followed by HPV 52 and 58. Among 43 patients with HPV 53, 24 (55.8%) showed persistent infection with the same HPV genotype. HPV 58 showed type-specific persistence after surgical treatment in 22 (29.7%) patients, while HPV 52 showed typespecific persistence in 27.5% (22/80) of patients. In contrast, HPV 16 and 18 showed relatively lower rates of type-specific persistence (19/128, 14.8%, and 2/23, 8.7%, respectively). In addition, among 43 patients infected with HPV 53, 36 (83.7%) were co-infected with other hrHPVs, while 40.6% (52/128) of those infected with HPV 16 were co-infected with other hrHPVs.
Fifty-seven patients (14.3%) showed residual/recurrent CIN during follow-up. Table 4 shows the risk factors for residual/recurrent CIN or CIN-2/3 after conization or LEEP. Post-menopausal status (OR, 3.969; 95% CI, 1.733–9.088; P<0.001) and infection with multiple hrHPV types (OR, 2.345; 95% CI, 1.109–4.958; P<0.05) were independent predictors of residual/recurrent CIN. In addition, risk of residual/recurrent CIN that was dependent on viral load was significantly greater in patients with a higher HPV load at baseline (OR, 2.430; 95% CI, 1.135–5.202; P<0.001), and in those with a higher HPV load at 18 months of treatment (OR, 5.351; 95% CI, 1.733–9.088; P<0.001). Of 15 patients with persistent or recurrent CIN-2/3 after conization or LEEP, CIN-2 lesions were found in 5 patients and CIN-3 lesions in 10 patients. Highly significant predicators of persistent or recurrent CIN-2/3 were menopause (OR, 4.31; 95% CI, 1.154–16.115, P<0.05) and higher HPV load after treatment for 18 months (OR, 4.24; 95% CI 1.201–14.963; P<0.05). In addition, initial CIN grade was also a predictor of residual/recurrent CIN. Patients with CIN-3 were more likely to have residual/recurrent CIN2+ after conization (OR, 10.87; 95% CI, 2.146–55.046; P<0.01). Compared to those with CIN-2 at enrollment, having CIN-3 was a risk factor for persistent or recurrent high-grade cervical precancerous lesions, although CIN-2 but not CIN-3 was a risk factor for persistence of hrHPV.

Logistic regression results for predicting the residual/recurrent cervical intraepithelial neoplasia (CIN) or CIN-2/3 after conization or loop electrosurgical excision procedure (LEEP) (n=57)
Detailed characteristics of the 15 patients with residual/recurrent CIN-2/3 are provided in Table 5. The mean age of patients with residual/recurrent CIN-2/3 was 45.1 (25–63) years, which was older than the mean age of all patients (P<0.05). Of these 15 patients, 6 (40.0%) were post-menopausal. The most prevalent hrHPV type was HPV 33, detected in 5 (33.3%) patients, followed by HPV 16 in 4 (26.7%), HPV 18 in 2 (13.3%), HPV 31 in 2 (13.3%), and HPV 52 in 2 (13.3%). Most residual/recurrent CIN-2/3 patients had a viral copy number above 102, except for 1 patient. Eight patients (53.3%) were infected with a single hrHPV type while the remaining 7 (46.7%) patients were infected with multiple hrHPV types. HPV genotyping revealed that 13 of the 15 patients (86.7%) remained positive for the same hrHPV at follow-up, while 2 (13.3%) patients were positive for a different hrHPV at follow-up from the type detected at enrollment. Persistent infection with HPV 16 was associated with a significantly increased risk for residual/recurrent CIN-2/3 compared to other types of HPV (OR, 3.422; 95% CI, 1.092–10.728; P<0.05). Among the 15 patients with residual/recurrent CIN2/3, the histopathologic finding was CIN2 in 3 (20.0%) and CIN-3 in 12 (80.0%) at enrollment. The mean time to diagnosis of residual/recurrent CIN-2/3 was 9.1 (2.1–23.1) months.
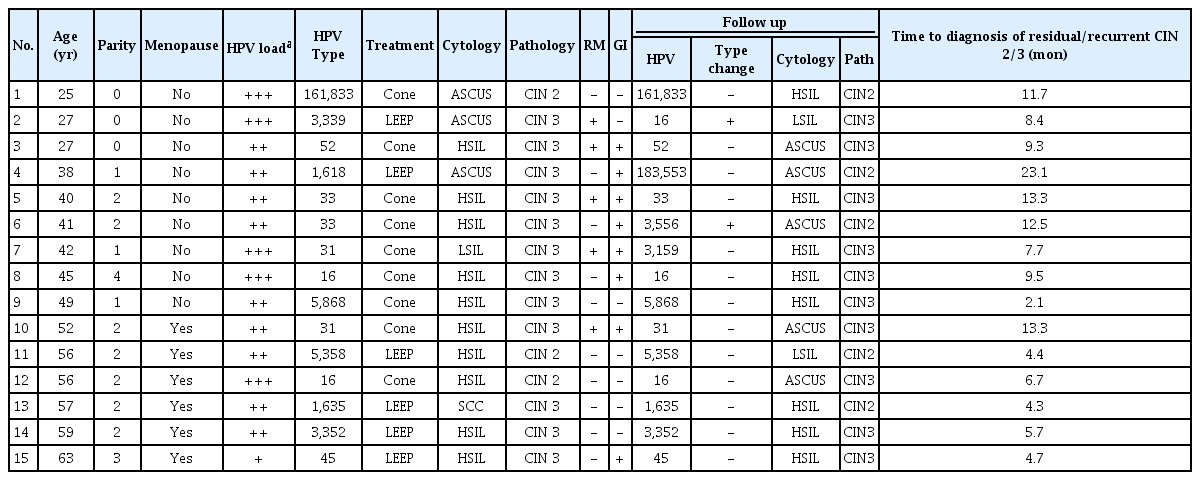
Characteristics of women showing residual/recurrent cervical intraepithelial neoplasia (CIN)-2/3 after treatment
Discussion
We aimed to determine which factors affect hrHPV persistence and residual/recurrent CIN after conization or LEEP. There was a significantly increased risk for persistence of hrHPV in patients with high preoperative HPV load and multiple hrHPV types. In addition, patients diagnosed with CIN-2 were at higher risk for hrHPV persistence than those diagnosed with CIN-3. HPV 16 was the most prevalent hrHPV genotype however; we found relatively higher persistence rates of HPV 53, 58, and 52 than HPV 16 or 18. We also found increased risk for residual/recurrent CIN-2/3 in patients who were postmenopausal or had higher postoperative HPV load. Patients with CIN-3 were at higher risk for residual/recurrent CIN-2/3 than CIN-2. The risk of residual/recurrent CIN-2/3 was higher in patients with persistent infection with HPV 16 than other HPV types. Our data support the usefulness of hrHPV genotyping and viral load testing before and after conization or LEEP to manage patients with CIN.
Consistent with previous studies, we observed that 38.7% of patients were positive for hrHPV after conization or LEEP [19,20]. However, the range of hrHPV persistence rates previously reported (7.8–17.4) were lower than what we observed [11,14,21]. The higher persistence rate in our study compared to other studies may be due to different definitions of hrHPV persistence. We defined hrHPV persistence as the presence of hrHPV at the first follow-up visit after surgery, whereas others had different follow-up intervals or defined persistence as positive hrHPV results at 2 or more consecutive visits. Kim et al. [11] detected persistent hrHPV infections in 45.6% of patients who had undergone LEEP with a negative resection margin at 3 months post-surgery, and 14.3% of patients at 6 months post-surgery. In the present study, 7.6% of all patients (15 of 398) were diagnosed with residual/recurrent CIN-2/3 and 9.7% of patients in the hrHPV persistence group (15 of 154) were diagnosed with residual/recurrent CIN-2/3. The median time to diagnosis of residual/recurrent CIN-2/3 was 9.7 months (2.1–23.1).
In our study, viral load was significantly associated with persistence of hrHPV and residual/recurrent CIN-2/3. Similarly, in a French cohort, patients with high viral load were more likely to have persistent hrHPV infections after conization than patients with lower viral load [22]. In addition, postoperative viral load was a predictor of residual/recurrent CIN-2/3. Previous literature found that higher hrHPV viral load at the 6-month follow-up visit was a significant risk factor for residual/recurrent CIN after conization or LEEP [23], which corresponds well with our findings. We found that infection with multiple hrHPV types before treatment increased the risk of persistence of hrHPV This corresponds well with previous research that demonstrated that infection with multiple hrHPV types has not only been found to be associated with increased risk of persistence hrHPV but also CIN-2/3 [24]. Individual hrHPV types function independently in CIN lesions and infection with multiple strains should be interpreted as having a cumulative effect, rather than a synergistic effect [25]. This is consistent with our finding that infection with multiple hrHPV types was associated with hrHPV persistence rather than residual/recurrent CIN-2/3.
Unexpectedly, we found that HPV persistence rates after treatment were higher in patients with CIN-2 than those with CIN-3, which is inconsistent with a previous study report [19]. Although the association between the severity of the cervical precancerous lesion and the risk of persistence is still unknown, patients with lower grade cervical lesions have been shown to have a higher viral load than those with CIN-3 [26]. Higher grade cervical lesions have been shown to contain lower viral DNA loads due to the presence of more immature and dysplastic squamous cells than lower grade lesions [26]. In our study, and consistent with previous findings, although patients with CIN-2 were more likely to show persistence of hrHPV after conization or LEEP, CIN-3 patients were at higher risk for recurrence of CIN-3 than CIN-2 [27].
In multivariate analysis, the hrHPV persistence rates were not affected by the status of resection margin (P=0.528), however a positive resection margin was associated with a 1.94-fold higher risk of hrHPV persistence (P<0.05) in univariate analysis. As several previous studies have pointed out [13,20,28,29], a positive resection margin is the most significant risk factor for predicting hrHPV persistence and residual/recurrent CIN-2/3. However, a negative resection margin does not always indicate complete excision due to the possibility of multifocal lesions. Sarian et al. [3] investigated the association between patient characteristics and hrHPV persistence, and demonstrated using multivariate analysis that smoking and patient age above 35 years were associated with persistent HPV, while a positive resection margin was not. They noted that positive endocervical margins were strongly affected by patient age (>35 years) because of the tendency for the squamous-columnar junction to be deeper inside the cervical canal after menopause. This finding indicates that the association between patient age and resection margin should be taken into consideration in statistical analyses of future studies.
We found that patients infected with HPV 53, HPV 58, and HPV 52 were at relatively higher risk for HPV persistence after treatment than those infected with other HPV types. One previous study [30] reported that α6 species of HPV (HPV 53, 56, 66) were less carcinogenic than other species of hrHPV, as well as being a low risk for progression despite persistence. Persistence of HPV 53 can be explained by the infection of tissues outside the precancerous lesion that are not causally related to the lesion. This may indicate that HPV 53 might not be causally involved, but might be a bystander [1,15]. HPV 52 is the most common type found in CIN-2, while HPV 16 is the most common type in CIN-3 and cervical cancer [30]. HPV 52 is also the most prevalent type in HIVinfected women [31] and is most frequently detected with HPV 16 [32]. Consistent with the most common persistent hrHPV types in our study, So et al. [33] investigated the prevalence and distribution of HPV genotypes in South Korea and reported that the most common types were HPV 53, followed by HPV 52 and HPV 58. In other words, our findings that the above 3 types of hrHPV were the most frequent types in patients with CIN might be due to their tendency to persist after surgical treatment. In agreement with our findings, Gosvig et al. [15], also found that the persistence rate for HPV 16 was lower than that of other carcinogenic HPV types after excision. Since HPV16 and HPV18 are known to be some of the most oncogenic subtypes, they could cause larger lesions, which would be associated with larger ranges of excision.
In our study, 15 patients were diagnosed with residual/recurrent CIN-2/3 during the follow-up period. Among them, 13 patients had persistent infection with the same hrHPV genotypes that they were originally infected. In addition, persistent infection with HPV 16 was significantly associated with residual/recurrent CIN-2/3 (P<0.05). Kang and Kim [34] found that patients with persistent infection with the same hrHPV types pre- and post-surgery, and HPV 18, were at high risk for recurrent CIN-2/3. Similarly, Söderlund-Strand et al. [35] reported that of 5.1% of patients diagnosed with residual/persistent CIN-2/3, all had the same type-specific hrHPV before and after surgery. In other studies, no recurrence was found among patients infected with newly-detected hrHPV types [36]. These results suggest that special attention should be paid to persistent infection after conization or LEEP with the same hrHPV type as was present before surgery.
The association between patients’ age and HPV persistence is still controversial. While, some previous studies found no correlation between patients’ age and HPV persistence or recurrent CIN after LEEP [37,38], one study reported that older patients with CIN lesions were at higher risk for HPV persistence [19]. In our study, menopause was a risk factor for persistent/recurrent CIN or CIN2+ after surgical treatment. The association between menopause and CIN persistence/recurrence may be explained by the fact that the squamouscolumnar junction of post-menopausal women is deeper within the cervical canal than that of pre-menopausal women. This location change in post-menopausal women would consequently interfere with complete hrHPV eradication or CIN removal due to limited resection depth. In addition, postmenopausal women may have a decreased immune response to HPV infection compared to pre-menopausal women [39].
The strengths of this study include our ability to perform HPV genotyping of all patients before and after conization or LEEP. Consequently, we could assess the associations between patient characteristics, including hrHPV types, hrHPV persistence, and residual/recurrent CIN-2/3, accurately. The limitations of our study include its retrospective design, relatively small sample size, and short follow-up duration. However, Elfgren et al. [40] reported that clearance of HPV DNA was rapid and usually occurred within 6 months of treatment, with little additional clearance after 6 months, therefore a longer term follow-up may not have altered our findings. In addition, the patient’s desire to become pregnant in future, could have influenced the cone depth or width during surgery; however, we could not consider this in our analysis. Finally, other factors affecting hrHPV persistence, or residual/recurrent CIN, such as a history of social behavior including smoking, were not evaluated.
In conclusion, our study contributes to the knowledge of the postoperative progress of hrHPV infection and CIN recurrence. We demonstrated that preoperative viral load and infection with multiple hrHPV types are important predictors of hrHPV persistence. HPV 53 was the most persistent type, whereas infection with HPV 16 was associated with the highest risk for residual/recurrent CIN-2/3. Post-menopausal women need to be monitored closely because of their high risk for residual/recurrent CIN. Longer-term and larger-scale studies are necessary to validate our results.
Notes
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Ethical approval
This study was approved by the Institutional Review Board of Korea University Guro Hospital (No. 2019GR0123).
Patient consent
Anonymized and de-identified information for participants was used for analysis, so the requirement for informed consent or parental permission was waived.