Current techniques used to perform surgery for anterior and posterior vaginal wall prolapse in South Korea
Article information

Abstract
Objective
This study aimed to evaluate the current surgical techniques for anterior and posterior vaginal wall prolapse repair in South Korea.
Methods
A web-based questionnaire survey was sent to 780 members of the Korean Society of Obstetrics and Gynecology. The items assessed in the questionnaire were the demographic characteristics and current surgical techniques used for the correction of anterior and posterior vaginal wall prolapse.
Results
The response rate was 16%. There were variations in the suture materials and methods used for anterior and posterior colporrhaphy. Most respondents used only rapid absorbable suture materials to plicate the fibromuscular layer and close the mucosal layer of the anterior and posterior vaginal wall. Simple interrupted sutures are the most popular suture method for both the fibromuscular and mucosal layers. Thirty-one and eleven percent of the respondents used mesh for surgical correction of anterior and posterior vaginal wall prolapse, respectively. Concomitant perineorrhaphy was routinely performed with posterior vaginal wall repair by 42% of the respondents, whereas 58% performed perineorrhaphy only in cases with perineal defects.
Conclusion
There is considerable diversity in the current surgical techniques for anterior and posterior vaginal wall prolapse repair in Korea. Further research is required to standardize the surgical techniques.
Introduction
Surgical repair of pelvic organ prolapse (POP) is prevalent in 11% of women, requiring surgery at least once during their lifetime [1]. The anterior vaginal wall is the compartment most commonly affected by prolapse, and the risk of recurrence is approximately 40% after surgical correction [1–3]. Surgical correction of posterior vaginal wall prolapse is estimated to be performed in approximately half of the patients who undergo surgery for POP [1–3].
Although anterior or posterior colporrhaphy is considered a standard procedure to correct anterior or posterior vaginal wall prolapse worldwide, a detailed description of surgical techniques is not provided even in well-conducted randomized controlled trials, and no clear internationally relevant guidelines exist. The use of mesh repair is more controversial than the colporrhaphy [4,5]. Since the Food and Drug Administration (FDA) approved vaginal mesh for the surgical correction of POP in 2002, there has been a significant increase in mesh use for anterior and posterior vaginal wall prolapse repair. However, several studies have reported unsatisfactory surgical outcomes and poor long-term safety [6–9].
This study aimed to evaluate the current surgical techniques for anterior and posterior vaginal wall prolapse repair among Korean obstetrician-gynecologists registered in the Korean Society of Obstetrics and Gynecology (KSOG).
Materials and methods
The survey protocol was approved by the Institutional Review Board (International St. Mary’s Hospital, Catholic Kwandong University, reference number: IS19QISI0), and the requirement for informed consent was waived. A web-based questionnaire was developed to assess the current surgical techniques used to correct anterior and posterior vaginal wall prolapse (Supplementary File 1) [10]. We sent a web-based questionnaire via e-mail to 780 members of the KSOG in September 2019 after obtaining permission from the KSOG. To increase the response rate to the survey, a follow-up email was sent after an interval of a month asking members to respond to the survey; the surveys were carefully screened to avoid duplicate participation.
The items evaluated in the questionnaire were demographic characteristics including age, sex, subspecialty, surgical experience, surgical volume in each surgeon, and surgical techniques for anterior and posterior vaginal wall prolapse repair including suture materials, suture methods, use of mesh, and concomitant perineorrhaphy at the time of posterior vaginal wall prolapse repair. Data were analyzed using SPSS ver. 22 software (IBM Corp., Armonk, NY, USA). We analyzed our data using a series of one-way tables. A P-value <0.05 was considered statistically significant.
Results
One hundred twenty-six members (16%) responded to the survey. Table 1 presents the respondents’ demographic characteristics. Most respondents were male (68%) and had a subspecialty other than urogynecology (76%). Of the respondents, 16% completed a fellowship for prolapse surgery, 52% had more than 10 years of experience, and 14% had conducted more than 50 cases of prolapse surgery per year.

Respondents’ demographics (n=126)
Table 2 presents suture materials used for anterior and posterior colporrhaphy. There were variations in the suture materials used for anterior and posterior vaginal wall repair. Most respondents used only a rapid absorbable (RA) suture material, including polyglactin (Vicryl®; Ethicon, Somerville, NJ, USA; Polysorb®; Covidien, Mansfield, MA, USA); 85 (67.5%) and 114 (90.5%) respondents used it for the repair of the fibromuscular and mucosal layers, respectively. For the repair of the prolapsed posterior compartment, they also preferred to use an RA suture; 94 (74.6%) and 112 (88.9%) respondents used it for the repair of the fibromuscular and mucosal layers, respectively. The second most preferred option was a delayed absorbable (DA) suture material, including polydioxanone (PDS II®; Ethicon) and glyconate (Monosyn®; B. Braun Surgical SA, Rubi, Spain); 13 (10.3%) and six (4.7%) used it for the repair of the fibromuscular and mucosal layers of the anterior vaginal wall, and 14 (11.1%) and eight (6.3%) used it for the repair of fibromuscular and mucosal layers of the posterior vaginal wall, respectively.

Suture materials used for anterior and posterior colporrhaphy
Table 3 presents suture methods used for anterior and posterior colporrhaphy. There were also variations in the suture methods used for anterior and posterior vaginal wall repair. Most respondents used a simple interrupted suture method to plicate fibromuscular layer and close mucosal layer of anterior and posterior vaginal wall. The second most preferred option for the plication of the fibromuscular layer was the horizontal mattress interrupted method; 22 (17.5%) used this method for both the anterior and posterior vaginal walls. For closure of the mucosal layer, the second most preferred option was a continuous locking suture method; 38 (30.2%) and 45 (34.9%) used this method for the anterior and posterior vaginal walls, respectively.
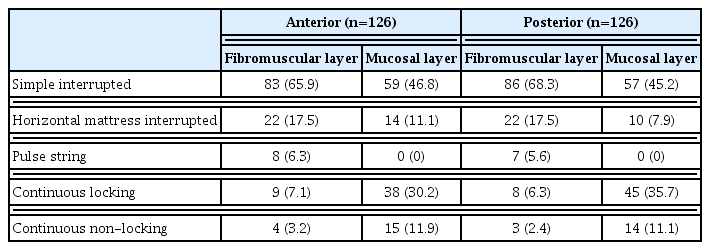
Suture methods used for anterior and posterior colporrhaphy
Thirty-nine (31%) and 14 (11%) respondents answered that they have used mesh for surgical correction of anterior and posterior vaginal wall prolapse, respectively. Concomitant perineorrhaphy was routinely performed with posterior vaginal wall repair in 53 respondents (42%), whereas 73 (58%) performed perineorrhaphy only in cases with a perineal defect.
Discussion
To our knowledge, this is the first web-based questionnaire to evaluate current surgical techniques for anterior and posterior wall repair in South Korea. Various surgeries are used to correct prolapse [2]. The procedures for anterior vaginal wall repair include colporrhaphy, graft and/or fascial plication, and paravaginal repair. Traditionally, colporrhaphy is the most commonly performed procedure to correct anterior and/or posterior vaginal wall prolapse [11,12].
Anterior and posterior colporrhaphy involves the midline plication of fibromuscular layers (pubocervical/rectovaginal fascia) of the anterior and posterior vaginal wall [13–15]. Various suture materials and methods are used in these procedures [13]. Interrupted sutures using absorbable suture materials are the most preferred suture technique for anterior colporrhaphy [13], which is consistent with our findings. There are two types of absorbable suture materials, RA and DA. RA suture materials lose their tensile strength within 14 days at least and total strength within 8 to 12 weeks [14,15]. DA suture materials maintain 50% of their tensile strength for up to 21 days and are not absorbed until 6 to 8 months [15]. Several studies have addressed the effects of RA and DA sutures on the anterior and posterior colporrhaphy. A randomized controlled trial found no significant difference in prolapse symptom scores between the groups at the 2-year follow-up, although the prolapse-related quality-of-life score was significantly better in the RA (Vicryl®) suture group than in the DA (PDS®) suture group for plication of the fibromuscular layer in the anterior and posterior colporrhaphy [16]. One retrospective cohort study also found no difference in the recurrence rate according to the type of suture (RA vs. DA) for plication of the fibromuscular layer in women who underwent anterior colporrhaphy in addition to the Manchester Fothergill procedure or vaginal hysterectomy [17]. In contrast, another prospective cohort study reported that the use of a DA suture for plication of the fibromuscular layer decreased the rate of symptomatic recurrence after anterior colporrhaphy compared with the use of RA sutures. However, comparing early postoperative complications between groups using RA and DA sutures for vaginal epithelial plication, the choice of suture material did not affect post-operative results and symptoms in posterior colporrhaphy [18]. Mizon and Duckett [19] reported that offensive vaginal discharge was more common in the RA suture group than in the DA suture group, although this did not result in an increased use of healthcare resources.
A few studies have evaluated the effect of the use of non-absorbable suture material for plication of the fibromuscular layer in colporrhaphy. Zebede et al. [20] reported that the use of nonabsorbable suture material for apical fixation with anterior colporrhaphy improved anatomic correction compared to the use of absorbable suture material. However, exposure to nonabsorbable sutures occurred in 15% of patients, and 40% required suture trimming to treat the exposure [20]. The use of nonabsorbable suture material in posterior colporrhaphy has also been reported to be associated with a higher rate of suture erosion/wound dehiscence than the use of absorbable suture material (31% vs. 9%) and the need for additional surgical intervention (16% vs. 0%) [21].
Synthetic mesh is a useful tool for reinforcing tissue strength and preventing prolapse recurrence. However, it is associated with high rates of adverse outcomes and disastrous long-term complication [5]. As the level of concern for mesh-related complications increased, the FDA reclassified transvaginal mesh from a class II (moderate-risk) to III (high-risk) device in 2016 [22]. More recently, in April 2019, the FDA ordered all manufacturers of surgical meshes intended for transvaginal repair of anterior compartment prolapse to stop selling and distributing their products immediately [23]. In our study, 39 (31%) and 14 (11.1%) surgeons still used mesh for anterior and posterior vaginal wall prolapse repairs, respectively.
Perineorrhaphy is a common surgery, either as a standalone operation or in conjunction with other surgical repairs for POP. Perineorrhaphy is thought to reinforce the perineal body, which may augment pelvic support because the perineal body provides a portion of the level III support of the uterus and vagina [24]. It is often performed for cosmetic reasons as well as to prevent recurrent prolapse, treat pain, and improve sexual function [24,25]. Despite this, there is no evidence to support this procedure. While some surgeons recommend it routinely include perineorrhaphy at the time of posterior vaginal wall repair, others include it on an “as needed” basis, depending on intraoperative findings [26]. Our survey showed that 53 surgeons (42.1%) “always” performed the procedure and others responded on an “as needed” with perineal defects.
To the best of our knowledge, this is the first study to reveal substantial surgical techniques for anterior and posterior vaginal wall prolapse repair in Korea. However, the study has a limitation. Our survey findings had sampling bias. We conducted the survey with the help of the members of the KSOG via e-mail. Our data indicated that most respondents were from tertiary medical centers. Current surgical techniques may be more representative of academic practice than general practice in Korea.
In conclusion, there were variations in suture materials and methods used for anterior and posterior colporrhaphy in South Korea. Most surgeons prefer to perform colporrhaphy using a simple interrupted suture method and a rapid absorbable suture material. Further studies are needed to assess whether these techniques influence surgical outcomes for the standardization of surgical techniques.
Notes
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Ethical approval
The survey protocol was approved by the Institutional Review Board (International St. Mary’s Hospital, Catholic Kwandong University, reference number: IS19QISI0).
Patient consent
Written informed consent and the use of images from patients are not required for the publication.
Funding information
This work was supported by a grant from the Korean Urogynecologic Society.
Supplementary material
Supplementary File 1 associated with this article can be found online at https://doi.org/10.5468/ogs.21352.
Supplementary File 1.
The survey for current technique of surgery for anterior and posterior vaginal wall prolapse in Korea