Risk factors differentiating mild/moderate from severe meconium aspiration syndrome in meconium-stained neonates
Article information
Abstract
Objective
The aim of this study was to compare the risk factors associated with mild/moderate meconium aspiration syndrome (MAS) with those associated with severe in meconium-stained term neonates.
Methods
Consecutive singleton term neonates (n=671) with meconium staining at birth from all deliveries (n=14,666) in our institution from January 2006 to December 2012 were included. Both maternal and neonatal variables were examined. Among the study population, for women who underwent the trial of labor (n=644), variables associated with labor were also examined. These variables were compared between the mild/moderate MAS group, the severe MAS group, and the MAS-absent group.
Results
MAS developed in 10.6% (71/671) of neonates with meconium staining at birth. Among the neonates with MAS, 81.7% had mild MAS, 5.6% had moderate MAS, and 12.7% had severe MAS. The presence of minimal variability was significantly increased in both the mild/moderate and the severe MAS groups. The frequencies of nulliparity, fetal tachycardia, and intrapartum fever were significantly increased in the mild/moderate MAS group, but not in the severe MAS group. While a longer duration of the second stage of labor was significantly associated with mild/moderate MAS, severe MAS was associated with a shorter duration of the second stage. Notably, low mean cord pH (7.165 [6.850-7.375]) was significantly associated with mild/moderate MAS, but not with severe MAS (7.220 [7.021-7.407]) compared with the absence of MAS (7.268 [7.265-7.271]).
Conclusion
Our data suggest the development of severe MAS is not simply a linear extension of the same risk factors driving mild/moderate MAS.
Introduction
Meconium aspiration syndrome (MAS) is a life-threatening disease that affects some neonates born with meconium staining [1,2,3,4,5,6]. Although the incidence of meconium-stained neonates is between 10% and 16% for full-term births [7,8,9,10], the actual rate of MAS among meconium-stained neonates is quite low, ranging from 0.10% at 37 weeks gestation to 0.31% at 41 weeks gestation [11,12]. This finding suggests that important predisposing factors, other than meconium staining itself, contribute to the development of MAS in neonates [13].
The causes of MAS are considered to be relatively complex; moreover, the pathophysiology of this disease has not yet been completely elucidated. Several common antepartum or intrapartum risk factors, as well as neonatal factors, have been reported to be associated with the development of MAS in neonates [8,14]. These factors include nulliparity, ethnicity (Pacific Islander, Indigenous Australian, African-American, and African), a gestational age longer than 41 weeks, intrapartum fever, abnormal fetal heart rate, low birth weight, low Apgar score, and mean low cord pH [15,16,17,18,19,20,21,22]. However, studies of some risk factors have yielded discrepant results, depending on the particular study. For example, Khazardoost et al. [17] found that the mode of delivery is not a risk factor for MAS; in contrast, Vivian-Taylor et al. [23] found that birth by cesarean section (CS) reduced the risk of MAS. On the contrary, other reports indicated that CS was associated with higher risk of MAS [24,25,26]. For example, Usta et al. [27] showed that CS increased the risk of MAS by up to three fold by logistic regression analysis. Similarly, the presence of thick meconium was found by to aggravate MAS Khazadoost et al. [17], whereas others have demonstrated the opposite effect [27,28].
Recent lines of evidence have suggested that severe MAS has a distinct pathophysiology compared with mild/moderate MAS [13,28]. Firstly, no correlation between the time and amount of meconium exposure and the severity of MAS was found [25,29,30]. Secondly, the clinical course of MAS could not be predicted from the severity of the radiologic findings of neonatal chest films [8]. Thirdly, the pathological changes in the alveoli of neonates with pulmonary hypertension, which are frequently associated with severe MAS, appear to be chronic rather than acute, presumably due to meconium aspiration during the peripartum period [13]. Moreover, autopsy studies have indicated that most meconium aspiration had already occurred in utero, before delivery [31,32]. Based on these studies, it has been hypothesized that severe MAS is caused by other processes, such as chronic asphyxia or infection, rather than the aspiration of meconium.
Considering these findings, we hypothesized that severe MAS does not develop as a linear extension of mild/moderate MAS, and that severe MAS is caused by distinct risk factors different from those that cause mild/moderate MAS. To test this hypothesis, we analyzed the differences in maternal, neonatal, and intrapartum risk factors between mild/moderate and severe MAS among term consecutive neonates with meconium staining at birth.
Materials and methods
This was a retrospective study of patients treated at our institution from January 2006 to December 2012. Women with a gestational term of at least 37 weeks were included; however, women with multiple gestations, preterm deliveries, fetal deaths in utero, or other major anomalies were excluded. The percentage of meconium-stained neonates at birth and various risk factors for MAS were assessed. Risk factors were divided into three categories: 1) maternal variables (age, parity, gestational age at delivery, presence of oligohydramnios [amniotic fluid index <5]); 2) neonatal variables (weight, sex, presence of fetal growth restriction, Apgar score, grade of meconium staining, cord pH, presence of base excess at birth, and neonatal intensive care unit admission and duration); and 3) variables associated with labor (rupture of membrane to delivery interval, durations of first and second stages of labor, use of labor epidural anesthesia, use of oxytocin, use of prostaglandin E2 (PGE2), and the presence of intrapartum fever [≥38℃]). Predelivery fetal heart rate (FHR) patterns were also analyzed. Abnormal FHR patterns were defined by the following criteria: fetal tachycardia (>160 bpm), bradycardia (<110 bpm), and minimal variability during the last 3 hours before delivery [18]. All variables were thoroughly reviewed by a single investigator (WC). The severities of MAS were defined as follows: mild, requiring <40% oxygen therapy for <48 hours; moderate, requiring ≥40% oxygen therapy for at least 48 hours; severe, requiring assisted mechanical ventilation for more than 48 hours and is often associated with PPHN (Persistent Pulmonary Hypertension of the neonate) according to the criteria defined by Cleary and Wiswell [33]. The medical records of the neonates who met these categories were selected for a retrospective analysis of neonatal outcomes. Obstetrical, neonatal intensive care unit registry, and medical records were also reviewed for this study. These variables were analyzed to identify the risk factors that differentiated mild/moderate MAS from the absence of MAS, and the risk factors that differentiated severe MAS from the absence of MAS (mild/moderate group vs. MAS-absent group, severe group vs. MAS-absent group). In addition, the placental examinations were also performed by a single pathologist (JSK) in available cases and the presence of acute chorioamnionitis, funisitis, meconium-laden macrophages in the chorioamniotic membranes and vascular muscle necrosis of umbilical and chorionic vessels were assessed.
Differences between categorical variables were analyzed with the Pearson chi-square test and Fisher's exact test. Differences between continuous variables were analyzed with Tukey's range test and Student's t-test. P-values <0.05 were considered statically significant. All statistical analysis was conducted using the IBM SPSS ver. 20.0 (IBM Corp., Armonk, NY, USA) and continuous variables were described as mean±standard deviation.
Results
In total, 14,666 deliveries were performed at our institution from January 2006 to December 2012. Out of the delivered neonates, 732 (4.99%) were meconium-stained. After excluding patients with multiple gestations, preterm deliveries, fetal deaths in utero, and patients with major anomalies, 671 meconium-stained singleton neonates were included in the study. MAS developed in 10.6% (71/671) of these meconiumstained neonates. The severities of the MAS cases were as follows: mild, 81.7% (n=58); moderate, 5.6% (n=4); and severe, 12.7% (n=9). The mortality rate of neonates with MAS was 4.2% (3/71); all of these cases exhibited severe MAS.
We first analyzed the relationships between maternal and intrapartum variables, mild/moderate MAS, and severe MAS. Compared with the MAS-absent group, the mild/moderate MAS group had significantly higher frequencies of nulliparity, fetal tachycardia, minimal variability, and intrapartum fever, in addition to a longer duration of the second stage of labor (Table 1). In contrast, no significant differences in the prevalence of oligohydramnios or fetal growth restriction (FGR) in the mild/moderate MAS group compared with the MAS-absent group were observed. Similarly, no significant differences in the modes of delivery between the mild/moderate MAS group and the MAS-absent group were observed. As in the mild/moderate MAS group, the presence of minimal variability was significantly increased in the severe MAS group. However, the frequencies of nulliparity, fetal tachycardia, and intrapartum fever were not significantly increased in the severe MAS group compared with the MAS-absent group. Interestingly, emergency cesarean sections were more commonly performed in the severe MAS group compared with the MAS-absent group. Moreover, a shorter duration of the second stage of labor (33.0±9.3 vs. 89.0±3.5 minutes, P=0.063) was associated with severe MAS. This finding contrasts with the longer duration of the second stage of labor in the mild/moderate MAS group (133.0±13.87 minutes).
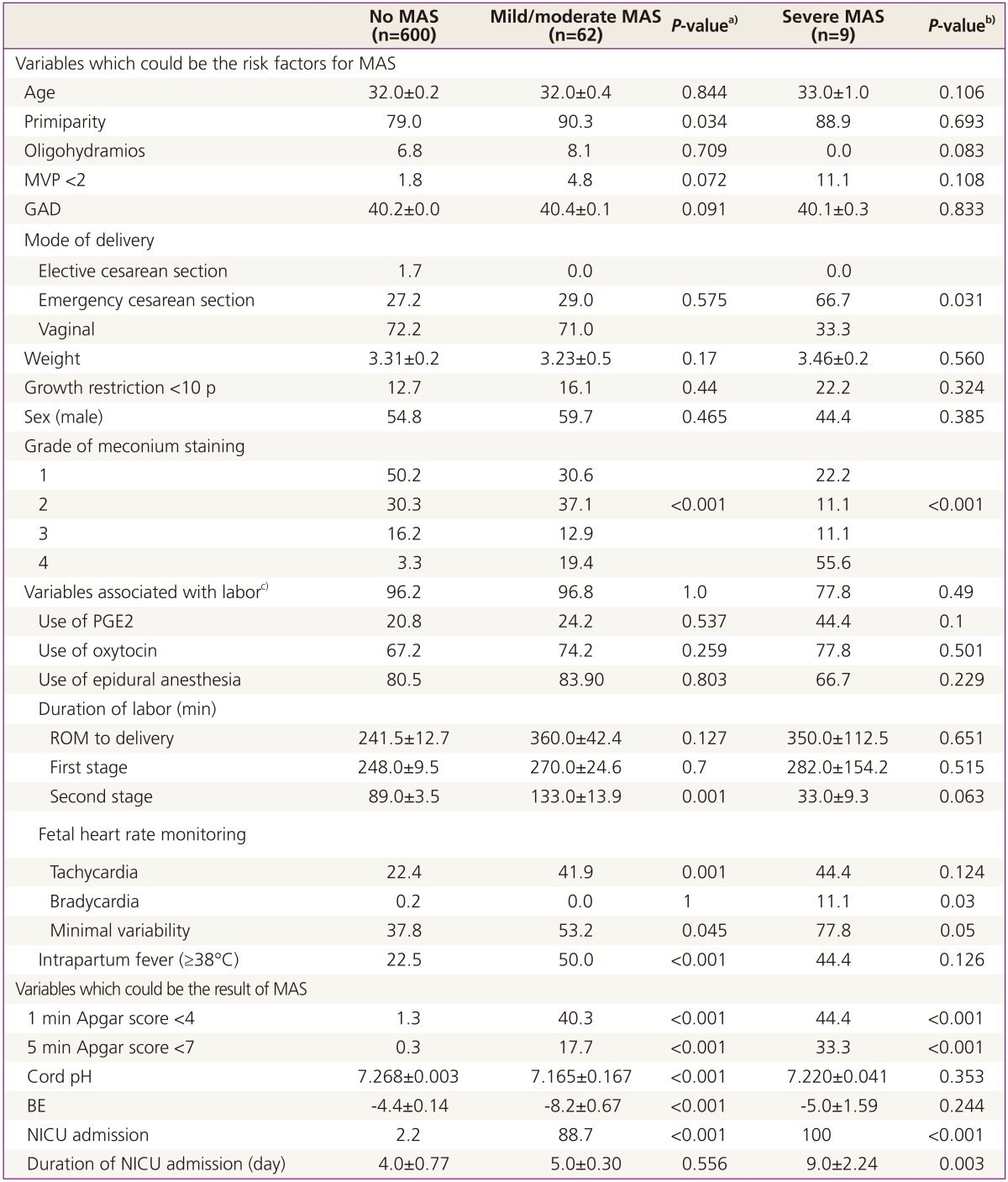
Clinical variables in mild/moderate MAS, severe MAS, and MAS-absent groups
Regarding the neonatal variables, low Apgar scores at 1 and 5 minutes were significantly more common in both the mild/moderate and severe MAS groups compared with the MAS-absent group. Notably, mean low cord pH was significantly associated with mild/moderate MAS (7.165 [6.850-7.375]), but not with severe MAS (7.220 [7.021-7.407]), compared with the MAS-absent group (7.268 [7.265-7.271]).
The maternal and neonatal characteristics of all cases of severe MAS are shown in Table 2. Two-thirds of all neonates with severe MAS were delivered by emergency cesarean section (5 cases were due to non-reassuring FHR, one case was due to arrest of dilatation). These 6 cases showed minimal variability before delivery (or at admission); moreover, the mothers in 2 of these 6 cases did not undergo the second stage of labor. Of the severe MAS cases, three resulted in neonatal deaths, yielding a high mortality rate of 33% in severe MAS cases. One mortality was due to PPHN; another neonate was a complicated quadriplegic cerebral palsy who died at home. The third neonate died of unknown causes. Among the surviving neonates, five were followed up for 2 years and were found to be neurologically normal. One neonate was lost for follow-up after discharge.
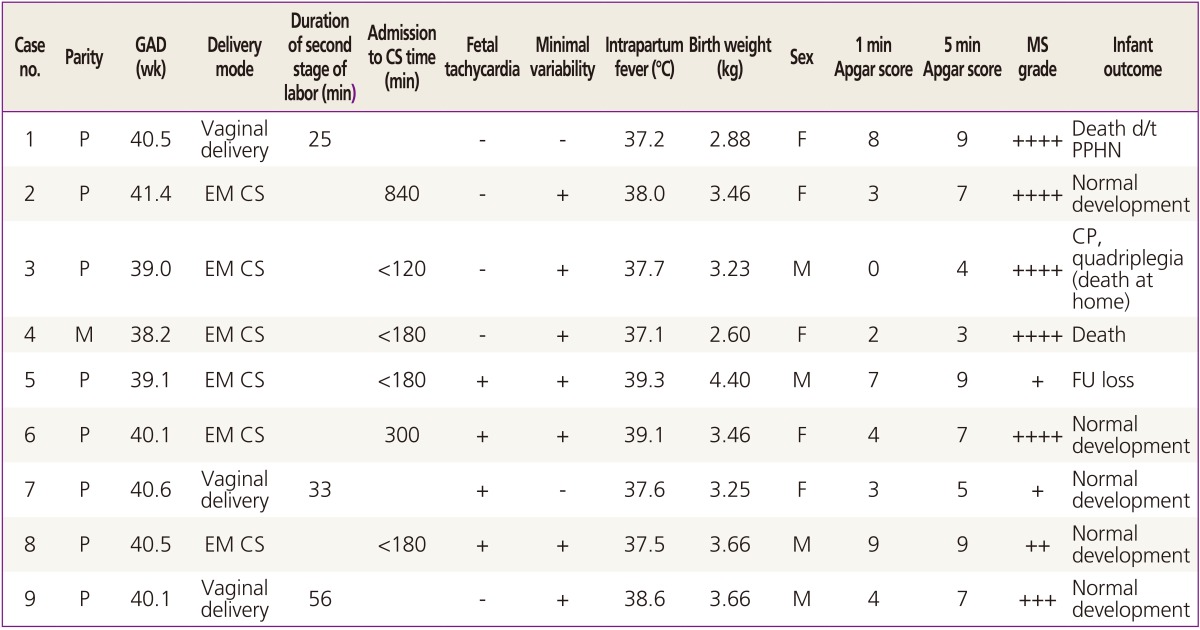
Clinical characteristics of severe meconium aspiration syndrome cases
Placental histologic findings in available cases from the study population are presented in Table 3. Compared with the MAS-absent group, severe MAS group was associated with higher rate of funisitis (42.2% vs. 100%, P=0.036). Other pathologic findings including acute chorioamnionitis, meconium-laden macrophages and vascular muscle necrosis were not significantly associated with mild/moderate or severe MAS.

Placenta pathology of mild/moderate MAS, severe MAS, and MAS-absent groups
Discussion
The data presented here identify distinct differences in the clinical risk factors associated with mild/moderate vs. severe MAS in meconium-stained term neonates. Regarding variables related to labor, mild/moderate MAS was found to be associated with significantly higher frequencies of minimal variability, fetal tachycardia, intrapartum fever (≥38℃), and a longer duration of the second stage of labor, compared with the absence of MAS. Among these variables, only minimal variability was a significant risk factor associated with the development of severe MAS. In contrast to mild/moderate MAS cases, the duration of the second stage of labor was reduced in severe MAS cases. Interestingly, mean low cord pH was significantly associated with mild/moderate MAS (compared with the absence of MAS), but not with severe MAS. Collectively, our data indicate that severe MAS is not a linear extension of the same risk factors driving mild/moderate MAS.
Since meconium-stained neonates accounted for 4.99% of all consecutive deliveries in our study, and MAS developed in 10.6% of these neonates, the prevalence of MAS in term pregnancies was calculated to be 0.53% in our study population. This finding is in accordance with other studies. For example, 5% to 12% of all neonates born through meconium-stained amniotic fluid have been found to develop MAS [33,34], and the incidence of MAS among term neonates has been reported to range from 0.43% to 1.8% [1,21]. Although we did not assess changes in the incidence of MAS throughout the study period, the incidence of MAS has been found to decrease each year [35]. The changing trend of performing elective inductions at 41 weeks, rather than at 42 weeks, has been suggested to be one of the most important contributing factors for decreasing the prevalence of MAS [21,23].
Diverse clinical risk factors for MAS, including black race, male sex, low birth weight, abnormal fetal heart pattern, cesarean section, low Apgar score, and thick meconium, have been reported to be associated with MAS in meconiumstained neonates [22,23,34]. However, different studies have yielded discrepant results regarding the risk factors for MAS. For example, it remains controversial whether birth by CS is a significant risk factor for MAS. Some studies demonstrated that birth by CS was not a significant risk factor for MAS [7,17], whereas others concluded that birth by CS was a significant risk factor for MAS [27]. A study by Fischer et al. [7] , which only included severe MAS cases (defined as cases treated by mechanical ventilation and/or continuous positive airway pressure), found that the CS rate was significantly higher in severe MAS cases compared with control cases. Our findings are consistent with this result. Likewise, conflicting evidence has also been obtained regarding the association between mean low cord pH and the development of MAS [16,25,36,37]. For instance, a study by Hernandez et al. [25], which included 82 cases of MAS, found that an umbilical arterial pH <7.20 was a predictor of prolonged ventilation in MAS. However, another study by Yeomans et al. [36] found only a poor correlation between the presence of meconiumstained amniotic fluid and umbilical cord pH. In fact, the incidence of true metabolic acidemia has been reported to be as low as 0.9% among all pregnancies with meconiumstained amniotic fluid [36]. In our study, the median cord pH in the mild/moderate MAS group was 7.165 [6.850-7.375], whereas the median cord pH in the severe MAS group was 7.220 [7.021-7.407]. Moreover, the incidence of metabolic acidemia (defined as a cord pH <7.0 and a base excess <-12) was 1.77% (11/622) among all meconium-stained neonates. Therefore, our data support the proposed hypothesis that nonhypoxic events or preexisting injuries are involved in the pathogenesis of severe MAS [38].
Some studies have found that thick meconium was associated with a high risk of developing MAS [22]; on the other hand, other groups have concluded that thick meconium staining had no relationship with the development of MAS [16]. We found that the presence of thick meconium was strongly associated with the development of MAS both in mild/moderate and severe form.
To the best of our knowledge, only one other study has investigated the risk factors differentiating mild/moderate MAS from severe MAS. In that study, Xu et al. [18] analyzed the risk factors for respiratory symptoms in 1,975 singleton neonates born through thick meconium-stained amniotic fluid, from a secondary analysis from randomized clinical trials of amnioinfusion. Variables related to clinical risk factors for mild, moderate/severe MAS, and late-onset respiratory distress were compared in detail with those of the reference group. This study found that marked tracing abnormalities requiring intervention, artificial membrane ruptures, and birth by CS were independent intrapartum risk factors for the development of moderate/severe MAS. We found that two variables associated with fetal heart rate abnormality, minimal variability and bradycardia, were associated with severe MAS. We also found that birth by CS was a significant risk factor for the development of severe MAS, but not for mild/moderate MAS.
It is particularly noteworthy that most (7/9) of the severe MAS cases in our study showed minimal variability, and that almost half (4/9) of the severe MAS cases presented minimal variability and required emergency cesarean sections within a few hours of admission. Among the mothers of neonates who developed severe MAS, those who underwent the second stage of labor and delivered vaginally had shorter second stages of labor compared with those of the control group (33.00±9.29 vs. 89.00±3.53). This observation contrasts with the finding that the duration of the second stage of labor was significantly longer in the mild/moderate MAS group (133.00±13.88). Cumulatively, our findings indicate that severe MAS is less dependent on the progression of labor than mild/moderate MAS; thus, some intrinsic factors may drive the progression of severe MAS. Consistent with this hypothesis, severe MAS has been proposed to originate in utero due to chronic causes, rather than being merely associated with intrapartum events [29,39].
There are few reports on the subject of placental histologic changes associated with MAS. A review of autopsy cases with MAS previously demonstrated that the inflammation of umbilical cord was present in 41% by Burgess and Hutchins [40]. It was also indicated that subacute or chronic in utero compromise was associated with eight infants who died of meconium aspiration [39]. In our study, we made efforts to uncover the placental histologic finings which may be relevant to the development of MAS and found that the presence of funisitis was significantly associated with severe MAS, but not with mild to moderate MAS, although only 37 cases of MAS (mild to moderate, 33 cases; severe, 4 cases) were subject to histologic assessment of placentas.
Our study did have some limitations. Although risk factors for the development of MAS were analyzed over a 7-year study period, the actual number of MAS cases was relatively small, particularly the number of severe MAS cases (n=9). Therefore, the statistical power of our study was somewhat limited. Secondly, since meconium staining at birth was used as the denominator, the incidence of MAS may have been overestimated compared with other studies, which generally included neonates with meconium-stained amniotic fluid instead [17,26,27]. Therefore, the incidences of mild/moderate MAS and severe MAS may not be directly applicable to clinical situations involving meconium staining via the amniotic fluid during labor, which are frequently encountered in obstetric practice. Furthermore, long-term neurodevelopmental outcomes were not determined for our entire study population. Although most neonates born with severe MAS (except one) were followed until reaching two years of age, many neonates born with mild/moderate MAS were discharged with complete recovery and were lost for follow-up.
Despite these limitations, our study had many strengths. One strength of our study is that we thoroughly examined multiple variables associated with labor, including rupture of membrane to delivery interval, the durations of the first and second stages of labor, the use of labor epidural anesthesia, the use of oxytocin, the use of PGE2, and the presence of intrapartum fever (≥38℃). Based on these data, we conclude that the only variables that increased the risk of mild/moderate MAS were a prolonged second stage of labor and the presence of intrapartum fever. Moreover, none of the laborassociated variables increased the risk for severe MAS, which was associated with all cases of neonatal mortality. We also collected extensive data regarding fetal heart rate monitoring. Taken together, this study provides useful information for the understanding the pathophysiology of MAS according to the severity and could help for the management of meconium stained labor in obstetrical practice.
Notes
No potential conflict of interest relevant to this article was reported.