Laterally extended parametrectomy
Article information
Abstract
Objective
To describe the laterally extended parametrectomy (LEP) surgical technique, emphasizing the main challenges of the procedure.
Methods
LEP was designed as a more radical surgical procedure aiming to remove the entire parametrial tissue from the pelvic sidewall. Its initial indications were for lymph node positive Stage Ib (current International Federation of Gynecology and Obstetrics 2018 Stage IIIc) and Stage IIb cervical cancer. Currently, with most guidelines recommending definitive radiochemotherapy for these cases, initial LEP indications have become debatable. LEP is now mainly indicated for removing tumors involving the soft structures of the pelvic sidewall during a pelvic exenteration, aiming to obtain lateral free margins. This expands the lateral borders of the dissection to not only the medial surface of internal iliac vessels, but also to the true limits of the pelvic sidewall.
Results
During LEP, the parietal and visceral branches of the hypogastric vessels are divided at the entry and exit level of the pelvis. Consequently, the entire internal iliac system is excised, and no connective or lymphatic tissue remain on the pelvic sidewall. The main technical challenges of LEP are caused by the difficulty in ligating large caliber vessels (internal iliac artery and vein) and the variable anatomic distribution of pelvic sidewall veins.
Conclusion
LEP is a feasible technique for removing pelvic sidewall recurrences, aiming to obtain surgical free margins.
The laterally extended parametrectomy (LEP) was designed as a more radical surgical procedure aiming to remove the entire parametrial tissue from the pelvic sidewall. Its initial indications were lymph node-positive stage Ib (current International Federation of Gynecology and Obstetrics 2018 stage IIIc) and stage IIb cervical cancer [1,2].
Nowadays, when most guidelines recommend definitive radiochemotherapy for these patients, the initial LEP indications are debatable [3,4]. LEP’s main indication is to remove tumors involving the soft structures of the pelvic sidewall during a pelvic exenteration [5], aiming to obtain lateral free margins. LEP expands the lateral borders of the dissection not only to the medial surface of internal iliac vessels but to the true limits of the pelvic sidewall [2].
During LEP, together with the visceral branches of hypogastric vessels, all the parietal branches are also divided at the level where the vessels leave or enter into the pelvis (Fig. 1). Consequently, the entire internal iliac system is excised, and no connective or lymphatic tissue remains on the pelvic sidewall [1].
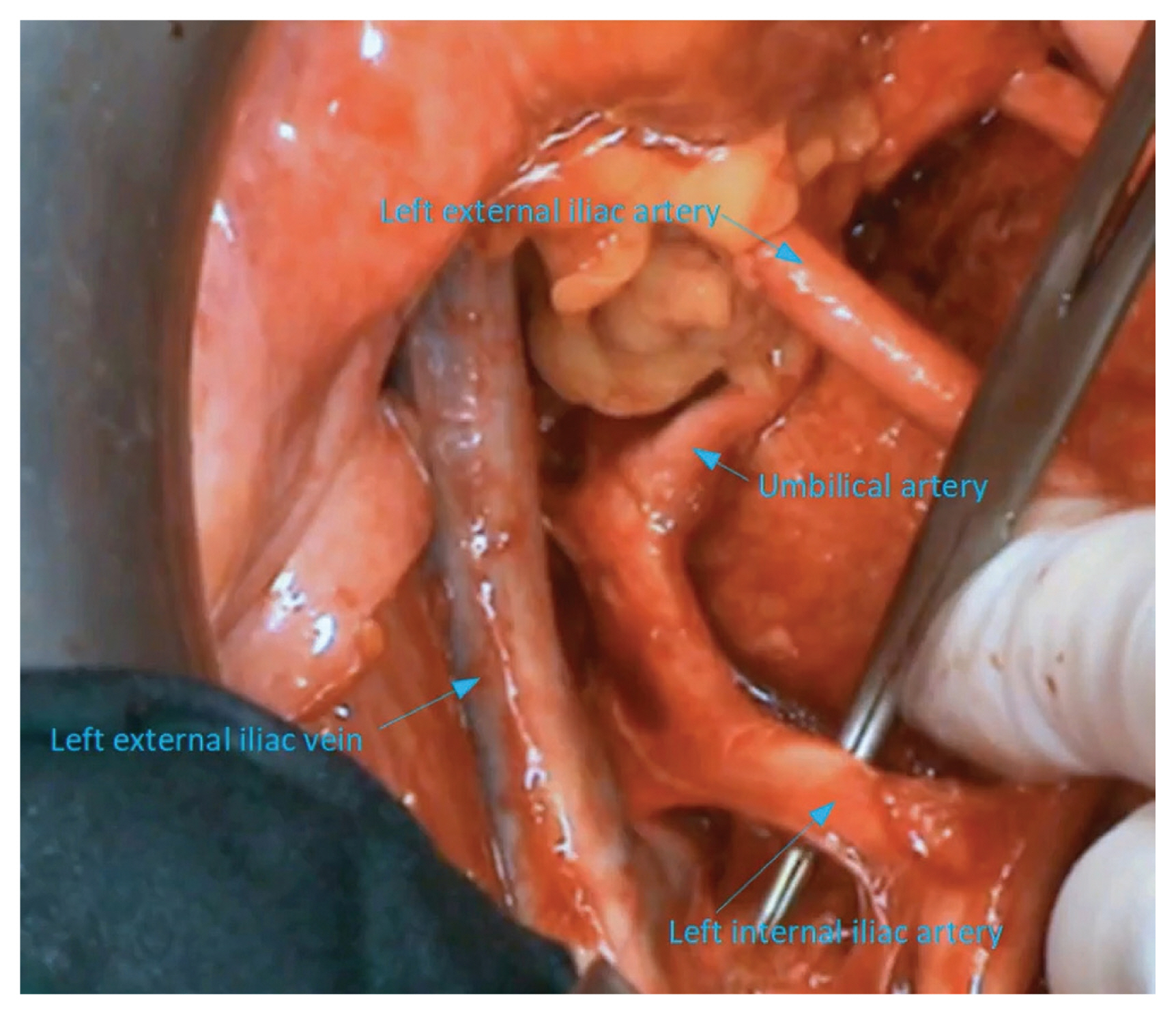
Left pelvic side wall after laterally extended parametrectomy in another patient.
The main technical challenge of LEP is caused by the difficulty to ligate large-caliber vessels (internal iliac artery and vein) and by the variable anatomic distribution of pelvic sidewall veins [2,6]. LEP is a feasible technique for removing pelvic sidewall recurrences, aiming to obtain surgical-free margins.
Video clip
Video can be found with this article online at https://doi.org/10.5468/ogs.21103.
Supplementary Information
Notes
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Ethical approval
The study was conducted under the approval of the appropriate Ethical Committee (ethical approval code: 34535) and written informed consent was obtained from the subject. The study was performed in accordance with the principles of the Declaration of Helsinki.
Patient consent
Written informed consent and the use of images from patients are not required for the publication.
Funding information
None.
Acknowledgements
To Andris Barabás, for his contribution with video editing. A different video of the same technique was presented at the 2020 xDigital Annual Global Meeting of the International Gynecologic Cancer Society.