



Introduction
Urinary incontinence is a worldwide problem that affects the millions of women. According to recent study, incidence of stress urinary incontinence is 30.4% in European women, 36.4% in American women [1]. Stress urinary incontinence is experienced by 31.6% to 47.1% of Korean women [2]. Tension-free vaginal tape (TVT) method has become mainstream in the surgical treatment of the stress urinary incontinence. Because the procedure is easier to perform than previous surgical method and that the cure rates are higher. The TVT method shortened operation time and recovery time, hospitalization period [3,4]. However, in the TVT method, a needle enters the retropubic space, and this could lead to complications, such as bladder perforation, urethra injury, retropubic hematoma [5,6]. In order to reduce the complication rate, the transobturator tape (TOT) method was presented as an alternative surgical technique in 2001 by Delorme [7]. In TOT method, a needle enters the obturator foramen. Anatomically, TOT method is not related with the retropubic space that reduces the risk of complications, therefore low complication rate and convenience of TOT method have resulted in a significant increase in usage of TOT [8]. However, the TOT method could rarely lead to uncommon complications, such as the obturator nerve and vessels injury, vulvar hematoma, obturator internus muscle abscess [9]. Significant bleedings have been scarcely reported in TOT procedure. The Gynecare TVT-Secur (Ethilcon, Somerville, NJ, USA) procedure was devised type of minimally invasive midurethral sling in 2006 [10]. This procedure intended to reduce complication rate by anchoring the tape in the obturator muscle instead of avoiding full needle passage. Significant bleedings have been scarcely reported in TOT and TVT-Secur (TVT-S) procedures. We presented two interesting cases of the pelvic arterial bleeding after the TOT procedure, a case of the pelvic arterial bleeding during the TVT-S procedure, its management.
Case report
1. Case 1
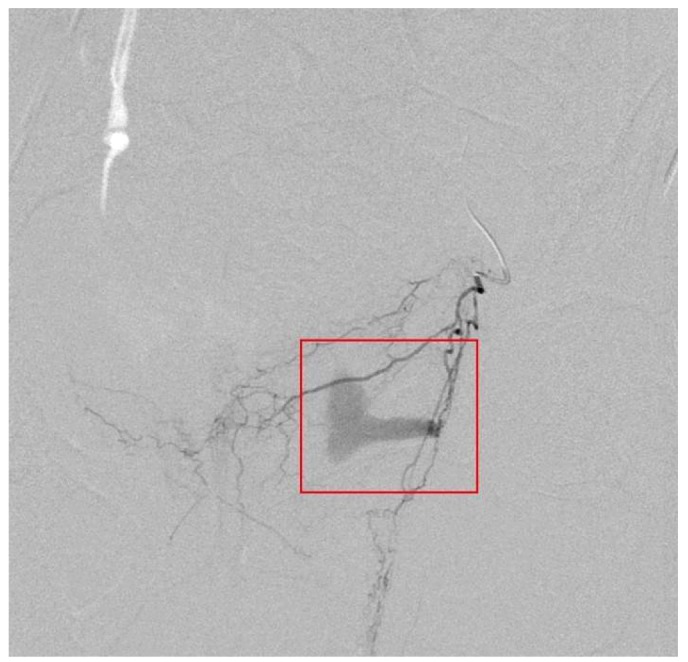
A 41-year-old woman was referred for vaginal bleeding. The previous day, she underwent a TOT procedure in a private gynecologic clinic. She urinated without difficulty and was discharged from the clinic. However, she presented with abdominal pain and voiding difficulty at the next day. She went to original clinic, they inserted foley catheter into her bladder to drain, she urinated 1,000 mL after foley catheter insertion. The original surgeon found hematoma on the vaginal wall and undertook hematoma removal. However, the vaginal bleeding persisted. Her hemoglobin dropped from a preoperative level of 15 to 9.6 g/dL. After packing with vaginal gauze, she was sent to our emergency care center. After arrival, she appeared pale and acute illness. Her blood pressure was 104/66 mmHg with tachycardia at 100/min. The left vaginal wall was found to be edematous and active bleeding. However, it was difficult to identify focus of bleeding. On the laboratory findings, the hemoglobin was 8.1 g/dL after two units of packed red cell transfusion, and coagulation factors, electrolytes, chemical batteries were within normal range. The patient was taken to angiographic room for embolization. Angiography showed extravasation of contrast from the upper vaginal branch of left internal iliac artery (Fig. 1). After super selection via microcatheter, selective embolization with glue were undertaken. Then extravasation of contrast was stopped. After embolization, vaginal bleeding was decreased and her vital signs stabilized. On post operation day 3, no evidence of active bleeding after embolization was observed on abdomen and pelvis computed tomography (CT). On post operative day 4, she reported no vaginal bleeding, she was discharged. Twelve days after her completed operation, she went to the emergency room, complaining of lower abdominal pain. Through the abdomen and pelvis CT scan, it turned out that the size of residual hematoma had decreased and extravasation didn't show up on the contrasted CT. She was discharged from the emergency room after receiving pain modulation. Fourteen days after the operation, we conducted a follow-up consultation and her abnormal pain had been mitigated. She did not show signs of any of the specific abnormalities. Her stress incontinence symptoms also improved in a follow-up consultation conducted in 3 months later.
2. Case 2
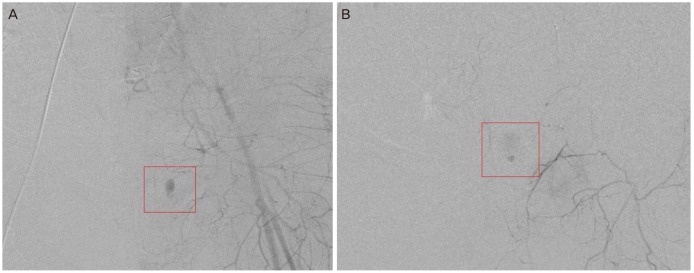
A 43-year-old woman was referred for low abdominal pain after TOT procedure in a private gynecologic clinic. Abdominal pain lasted for 7 hours after procedure and she went to our emergency care center. On arrival, she appeared pale and acute illness. Her blood pressure was 102/75 mmHg and heart rate was 95/min. She complained lower abdominal tenderness and rebound tenderness. Vagina and cervix were no specific findings in pelvic examination. Vaginal bleeding was scanty. After arrival, her hemoglobin was 12.6 g/dL and coagulation factors, electrolytes, chemical batteries were within normal range. Abdomen and pelvis CT showed a 10-cm-sized hematoma in left pelvic cavity with extravasation of contrast. Abruptly, her blood pressure dropped to 96/63 mmHg. Hemoglobin dropped from 12.6 to 10.9 g/dL. During resuscitated with intravenous fluid and two units of packed red blood cells, we made a diagnosis as retroperitoneal pelvic hematoma with active bleeding. She was taken to operation room for evacuation of hematoma and bleeding control. We found a large amount of hematoma in abdominal cavity and undertook hematoma removal. Although we tried to find bleeding focus but we couldn't, and bleeding persisted at pelvic wall. We sent her to our angiographic room for embolization to confirm pelvic vessel injury. Left iliac artery angiography showed extravasation of contrast from pubic branch of Left obturator artery (Fig. 2A). After use of glue, post embolization angiography showed remained bleeding foci. Left external iliac artery angiography showed extravasation of contrast from Left inferior epigastric artery (Fig. 2B). After insertion of microcoil and use of gelfoam, extravasation of contrast was stopped. After embolization, her vital signs stabilized and hemoglobin was 11.4 g/dL. Patient was given 8 units of packed red cells during her hospitalization. Since the overall amount of vaginal bleeding diminished, she had no longer complained of leakage symptom. She was discharged on postoperative day 5 without any complications. On postoperative day 11, she went to our emergency care center because she presented with lower abdominal pain. Abdomen and pelvis CT showed a size of residual hematoma decreased from 10 to 7 cm without contrast extravasation. On post operative day 13, she had no further symptoms.
3. Case 3
A 43-year-old woman underwent a TVT-S procedure in our gynecologic clinic. During operation, we found hematoma on the left anterior vaginal wall and active bleeding were observed from the incision in the suburethral portion. We undertook hematoma removal and tried to find bleeding focus. However we couldn't find a definitive bleeding focus, and bleeding persisted at vaginal wall. Patient was given 8 units of packed red cells and 3 units fresh frozen plasma during operation. We decided to undergo embolization for treatment of pelvic vessel injury. The patient was taken to angiographic room for embolization. No definite bleeding focus on left internal and left common iliac arterial angiography. Embolization of anterior trunk of left iliac artery using gelfoam was done. After embolization, the vaginal bleeding was stopped and her vital signs remained stable. On the following day, no vaginal bleeding was observed. She was discharged on postoperative day 7 without any complications.
Discussion
Various surgical methods have been developed to treat female stress urinary incontinence with minimum invasion. Soon after its presentation in 1996 by Ulmsten et al. [3]. TVT method became popular for the surgical treatment of stress urinary incontinence. Several studies have shown that the cure rates of TVT method are higher than previous surgical method [4]. Moreover the TVT method is easier to perform, and requires local anesthesia. However the TVT method has the risk of complication, such as bladder, bowel and vascular injury due to the blind passage of needle through the retropubic space [5,6]. The TOT method that involves passage of needle through the obturator foramen, was developed to reduce the disadvantage related to the passage of the sling through the retropubic space [11]. Short term clinical trials have concluded that the TOT method demonstrates better result than TVT method in terms of the rate of complication with similar cure rate of stress urinary incontinence [11]. The TVT-S was devised to reduce the risk of vascular, nerve, bowel injury, because needle does not through retopubic or obturator space in TVT secure procedure [10].
Up to now, reports of vascular injury after the TOT procedure are limited. Theoretically, TOT method may have a lower rate of vascular injury after procedure than the TVT method. Because a needle enters the obturator foramen rather than the retropubic space, passes on average 3cm inferior medial to the obturator artery in the TOT method [11]. However, we cannot exclude the possibility of vascular injury even after the TOT procedure [12].
These vascular injuries can be managed by conservative treatment because it does not go with hemodynamic instability. Rajan and Kohli. [13] reported two cases of pelvic hematoma after the TOT procedure. One patient received conservative management, and the other required CT guided drainage of the hematoma. Choi et al. [14] reported one case of pelvic hematoma following the TOT procedure, this patient was also managed conservatively. In case of instability of vital sign which is led by massive bleeding, or artery injury, surgical procedure is required. Some cases were reported that bleeding after TOT procedure is treated by embolization in Korea [15,16]. Park et al. [15] reported uterine arterial injury and hypovolemic shock after TOT procedure, which was successfully treated by selective embolization. Ku et al. [16] also reported uterine arterial injury and postoperative anemia after TOT procedure, which was treated by emoblization.
The strength of our current report is that we present a variety of clinical features in the three cases. In previously reported cases, retroperitoneal pelvic hematoma was presented with vaginal bleeding, while our patients detected by abdominal pain and voiding difficulty except last case [14,15]. Even if there is no vaginal bleeding, retroperitoneal pelvic hematoma should be considered if the patient presents with some other symptoms or vital sign instability.
The timing of embolization for arterial bleeding varies from intraoperative to one day after surgery. Consequently, when it is difficult to stop the bleeding by using compression or to find a bleeding focus, embolization must be considered, even if the operation is ongoing. If there is a chance of active bleeding, the possibility of embolization must also be considered, no matter how long it has been since the operation commenced. Furthermore, our current study patients were treated by pelvic arterial embolization due to not only uterine arterial injury, but also other arterial injuries, namely, a left obturator artery, left epigastric artery injury, and injury of the vaginal branch of the internal iliac artery.
There was no pelvic arterial bleeding following TOT procedure for 10 years in our gynecologic clinic. We assume the reason is that we could prevent massive bleeding by compression with vaginal gauze packing after TOT procedure. Almost bleedings following TOT procedure can be managed by compression. However, bleeding focus was not identified in third case. We decided to take embolization because the patient's vital sign was unstable, and massive transfusion was required for patient based on persistence of active bleeding. Bleeding was successfully controlled after pelvic arterial embolization. Therefore, angiography with embolization promptly could be considered a method to control bleeding when bleeding focus is not identified. Although the risk of vascular injury following TOT procedure is rare, we should not exclude the possibility. Early recognition of complication is important to management. We have to decide management plan promptly through imaging modalities such as pelvic CT scan, if an arterial injury is suspected. Pelvic arterial embolization is a preferable treatment choice for severe arterial bleeding after the TOT procedure.






")











