




Introduction
Preeclampsia (PE) is a multifactorial disorder that occurs during pregnancy and is characterized by hypertension and proteinuria after 20 weeks of gestation [1,2]. It brings about high morbidity and mortality in mothers and their babies, affecting 1-8% of pregnancies extending beyond 20 weeks [3]. Patients with severe PE require close monitoring for progression to an eclamptic event [4].
Historically, women with advanced age, obesity, nulliparity, underlying medical conditions, and assisted reproductive technology treatment are more likely to develop PE [5-8]. The overall incidence of hypertensive disorders during pregnancy has increased globally [9], while some high-income countries in northern Europe and Australia have reported a decreasing burden of the disease [10,11]. There are limited data regarding the recent epidemiology of mild and severe PE in high-income countries, where most pregnancies occur in women of advanced age. Here, we report trends in the incidence and risk of mild and severe PE among contemporary South Korean women.
Materials and methods
This is a retrospective observational study using the National Health Information (NHI) Database of NHI Service of South Korea, which covers approximately 97% of the Korean population. We identified a national cohort of 2,053,234 women who gave birth between January 2010 and December 2019 based on the childbirth treatment codes. Those without preconception health checkup data (n=300,570) were excluded. Women who had undergone a health examination at least once before their last menstrual period (which is estimated based on the date of childbirth [12]), and therefore had available baseline clinical data, were then selected among the pregnancy cases. We excluded women with a history of prior childbirth because we could not retrieve information on prior PE, an established risk factor for PE, for multiparous women who gave birth before 2010. Inclusion criteria were women who were between 20 and 49 years of age and nulliparous. This yielded a final study population of 1,317,944 women.
We included maternal age at birth, relative income level (in deciles), employment status, living in the Seoul metropolitan area, plurality, prepregnancy body mass index, prior history of smoking, fasting blood glucose level, and year of childbirth in the explanatory model. We identified patients who were diagnosed with PE during pregnancy based on the International Classification of Disease (ICD), 10th revision, codes (ICD-10: O14.0, O14.1, O14.2, and O14.9). We defined severe PE patients as those with a diagnostic code for PE as well as a prescription code for intravenous magnesium sulfate (MgSO4) [13,14], because its use to prevent eclamptic seizure is the essential feature of the “severity” of the condition. Mild PE was defined by the presence of only one diagnostic code.
Descriptive statistics were calculated based on the presence of mild or severe PE. Annual odds ratios (ORs) and 95% confidence intervals (CIs) for total, mild, and severe PE were computed adjusting for all the individual covariates. Effect modification by maternal age was assessed in the association between age and PE. We used the SAS statistical program (version 9.4; SAS Institute, Cary, NC, USA).
Results
Among the 1,317,944 nulliparous women who gave live births, the majority were aged <35 years (67.3%), had singleton pregnancies (97.4%), and lived outside of the Seoul capital area (74.1%). Income was lower than the national median in almost half of the population (44.9%). The risk of PE (3.4%) and severe PE (1.2%) was highest when maternal age was 45-49 years, which was almost three times higher compared to that in women 20-24 years old.
When the study population was classified by PE diagnosis, the proportion of women aged ≥35 years was higher in the mild (29.0%) and severe PE (32.7%) groups than in the no PE group (20.5%; Table 1). The distribution of maternal age was not different between the no PE, mild PE, and severe PE groups. Generally, women who were diagnosed with severe PE tended to be medical aid beneficiaries, showed the lowest income quartile, and had a higher likelihood for disability, multiple gestations, and impaired glucose intolerance, compared to those with a diagnosis of mild or no PE.
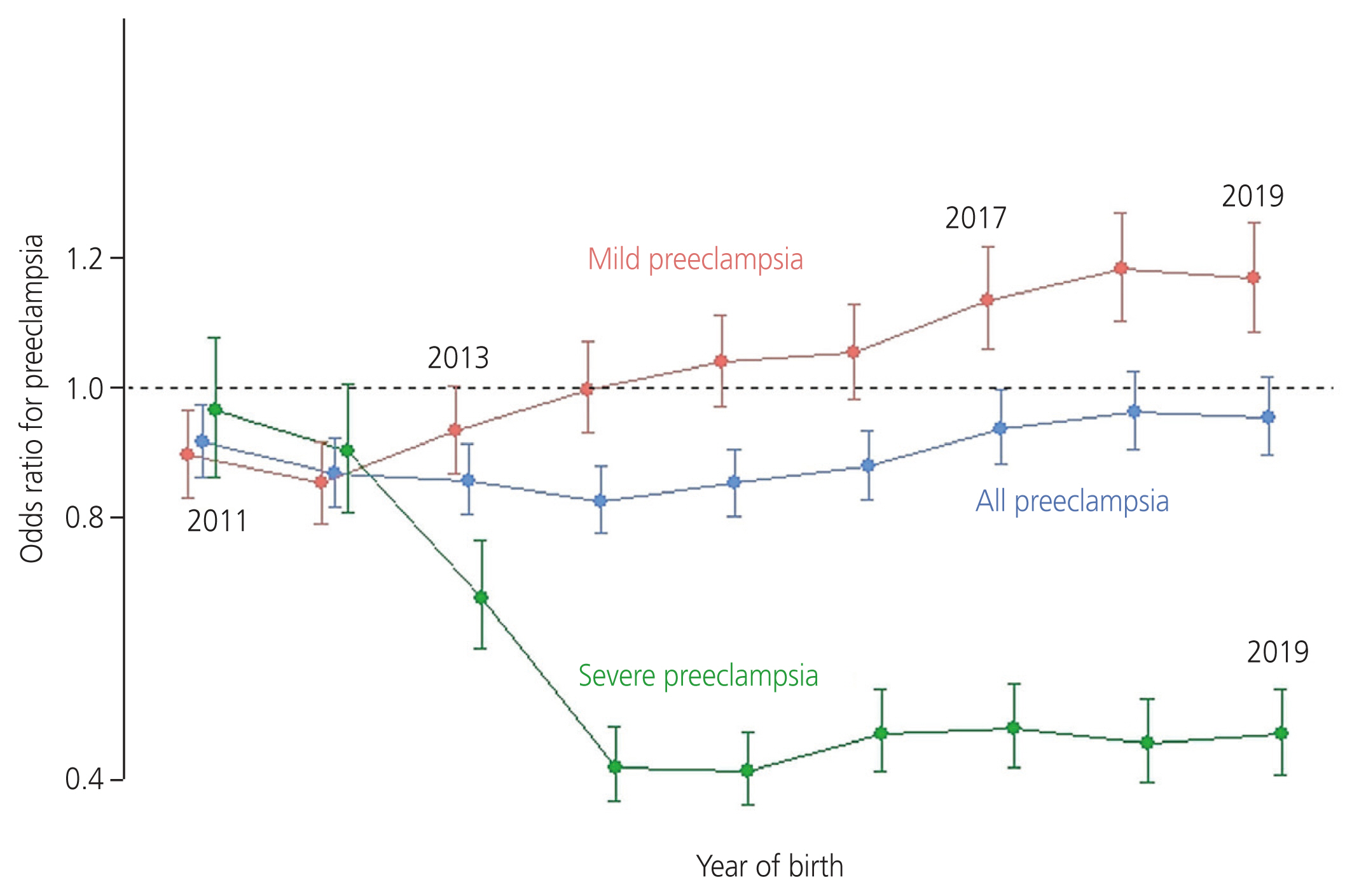
The overall cumulative incidences of mild PE and severe PE were 1.3% and 0.3%, respectively. Mild PE increased from 0.9% in 2010 to 1.4% in 2019 (P for trend=0.006), while severe PE decreased from 0.4% in 2010 to 0.3% in 2019 (P=0.049). The incidence of all types of PE (mild and severe) showed no linear change (P=0.514). Compared to that in 2010, the adjusted OR of severe PE was lower in 2013 (OR: 0.68; 95% CI: 0.60, 0.77) and beyond, while the OR of mild PE was higher in 2017 (1.14; 95% CI: 1.06, 1.22; Fig. 1) and beyond. The OR for all PE in the period 2011-2017 remained lower than that in 2010, and returned to the 2010 levels during 2018-2019. We assessed the effect of advanced age at birth on the association between the year of birth and PE. The trend of adjusted OR for all PE per year did not significantly differ between women aged <35 years and those aged ≥35 years.
Discussion
We observed different patterns in the incidence and risk of mild and severe PE in South Korean women over the past decade. Despite the overall increase in the number of older mothers, the crude incidence of all types of preeclampsia did not increase. When we adjusted for individual risk factors, the risk of mild PE increased, whereas that of severe PE decreased, suggesting that patients with mild PE have been less likely to progress to severe PE since 2010.
The decrease in severe PE can be attributed to reduced progression of mild PE to the severe form or to the physicians’ decision to induce childbirth in advance. As the annual incidence of induction of labor in nulliparous women decreased during the study period (from 22.8% in 2010 to 20.3% in 2019) [15], the decrease in severe PE would be less likely due to labor induction. The decreasing risk of severe PE may be explained by the widespread use of aspirin in high-risk pregnancies and the higher coverage of antenatal voucher programs provided by the South Korean government [16]. Because data on aspirin use during pregnancy were unavailable, we could not assess its impact. In South Korea, a universal voucher scheme was initiated in 2008 to alleviate the financial burden of pregnant women for antenatal care and birth services [17]. We previously reported a significant reduction in preeclampsia in the general population after the introduction of the voucher scheme, which remained significant after controlling for individual risk factors [14].
The results of the present study should therefore be interpreted with caution. There may have been a tendency toward overreporting by physicians, and misclassification or miscoding may have affected the results of this study. Given that the incidence of mild PE was reported to be 2.5-4 times higher than that of severe PE in prior studies [18-20], we believe that the possibility of misclassification would have been minimal. Second, our operative definition of severe PE based on the prescription of MgSO4 may have been affected by the recommendation of the United States. Food and Drug Administration against prolonged use of MgSO4 to stop preterm labor due to bone changes in exposed babies in 2013. However, given the consistent incidence of severe PE since 2012, we believe that the decreasing trend in the adjusted risk of severe PE is less likely to be attributable to this recommendation.
In conclusion, mild PE has been less likely to progress to the severe form since 2010. However, the overall risk of PE has not changed among contemporary South Korean women. Further studies identifying the factors that reduce the risk of progression to severe PE are needed to understand the epidemiological changes in this condition.






")











